
Page 10 - Journal of Laparoscopic Surgery
P. 10
Anburaja Mahalingam et al
animals were randomly divided into two equal groups (I and of blood vessels. Then, the vas deferens and spermatic artery-
II). In group I, laparoscopic vasectomy by cauterization and vein plexus were visualized. The vas deferens was identified
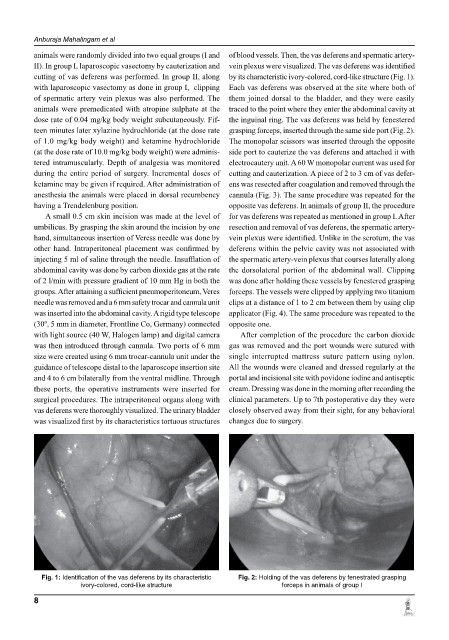
cutting of vas deferens was performed. In group II, along by its characteristic ivory-colored, cord-like structure (Fig. 1).
with laparoscopic vasectomy as done in group I, clipping Each vas deferens was observed at the site where both of
of spermatic artery vein plexus was also performed. The them joined dorsal to the bladder, and they were easily
animals were premedicated with atropine sulphate at the traced to the point where they enter the abdominal cavity at
dose rate of 0.04 mg/kg body weight subcutaneously. Fif- the inguinal ring. The vas deferens was held by fenestered
teen minutes later xylazine hydrochloride (at the dose rate grasping forceps, inserted through the same side port (Fig. 2).
of 1.0 mg/kg body weight) and ketamine hydrochloride The monopolar scissors was inserted through the opposite
(at the dose rate of 10.0 mg/kg body weight) were adminis- side port to cauterize the vas deferens and attached it with
tered intramuscularly. Depth of analgesia was monitored electrocautery unit. A 60 W monopolar current was used for
during the entire period of surgery. Incremental doses of cutting and cauterization. A piece of 2 to 3 cm of vas defer-
ketamine may be given if required. After administration of ens was resected after coagulation and removed through the
anesthesia the animals were placed in dorsal recumbency cannula (Fig. 3). The same procedure was repeated for the
having a Trendelenburg position. opposite vas deferens. In animals of group II, the procedure
A small 0.5 cm skin incision was made at the level of for vas deferens was repeated as mentioned in group I. After
umbilicus. By grasping the skin around the incision by one resection and removal of vas deferens, the spermatic artery-
hand, simultaneous insertion of Veress needle was done by vein plexus were identified. Unlike in the scrotum, the vas
other hand. Intraperitoneal placement was confirmed by deferens within the pelvic cavity was not associated with
injecting 5 ml of saline through the needle. Insufflation of the spermatic artery-vein plexus that courses laterally along
abdominal cavity was done by carbon dioxide gas at the rate the dorsolateral portion of the abdominal wall. Clipping
of 2 l/min with pressure gradient of 10 mm Hg in both the was done after holding these vessels by fenestered grasping
groups. After attaining a sufficient pneumoperitoneum, Veres forceps. The vessels were clipped by applying two titanium
needle was removed and a 6 mm safety trocar and cannula unit clips at a distance of 1 to 2 cm between them by using clip
was inserted into the abdominal cavity. A rigid type telescope applicator (Fig. 4). The same procedure was repeated to the
(30º, 5 mm in diameter, Frontline Co, Germany) connected opposite one.
with light source (40 w, Halogen lamp) and digital camera After completion of the procedure the carbon dioxide
was then introduced through cannula. Two ports of 6 mm gas was removed and the port wounds were sutured with
size were created using 6 mm trocar-cannula unit under the single interrupted mattress suture pattern using nylon.
guidance of telescope distal to the laparoscope insertion site All the wounds were cleaned and dressed regularly at the
and 4 to 6 cm bilaterally from the ventral midline. Through portal and incisional site with povidone iodine and antiseptic
these ports, the operative instruments were inserted for cream. Dressing was done in the morning after recording the
surgical procedures. The intraperitoneal organs along with clinical parameters. Up to 7th postoperative day they were
vas deferens were thoroughly visualized. The urinary bladder closely observed away from their sight, for any behavioral
was visualized first by its characteristics tortuous structures changes due to surgery.
Fig. 1: Identification of the vas deferens by its characteristic Fig. 2: Holding of the vas deferens by fenestrated grasping
ivory-colored, cord-like structure forceps in animals of group I
8