
Page 7 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 7
6 SECTION 1: Essentials of Laparoscopy
while not including the fascia may increase the rate of end of the Veress needle should be pointed toward anus
failed entry (Fig. 15). (Fig. 15). To prevent creation of preperitoneal slip of tip
■ ■Hold the Veress needle just over the previously incised of Veress needle, it is necessary that Veress needle should
site and insert it through the incision at a 45° angle be perpendicular to the abdominal wall. However, there
toward anus but keep perpendicular to the abdominal is a fear of injury of great vessels or bowel if Veress needle
wall. This can be only achieved by lifting the abdominal is inserted perpendicular to the abdominal wall. To avoid
wall adequately by left hand (Fig. 15). both the difficulty (creation of preperitoneal space and
■ ■While inserting the Veress needle feel for two “pops”. injury to bowel or great vessels), the lower abdominal wall
The first occurs when the needle passes through the should be lifted in such a way that it should lie at 90° angle
abdominal fascia and the second as it passes through in relation to the Veress needle but in relation to the body
the parietal peritoneum. More lateral access sites may of patient Veress needle will be at an angle of 45° pointed
have additional “pops” if more than one layer of fascia toward anus. Lifting of abdominal wall should be adequate
is traversed. so that the distance of abdominal wall from viscera should
■ ■As soon as the needle enters the peritoneal space, the increase. If less than required dose of muscle relaxant is
displaced hub of the needle will “click” as the protective given in muscular patient, lifting of abdominal wall may
sheath recoils to cover the end of the needle. After be difficult. In multipara patient, lifting lower abdominal
entering in abdominal cavity, the intra-abdominal wall is very easy.
needle will also move more freely than a needle within Several tests are available for confirming Veress needle
the abdominal wall. placement. These include one of the following:
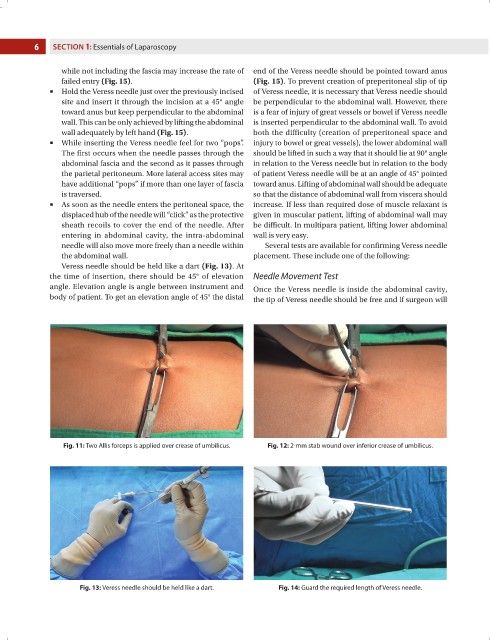
Veress needle should be held like a dart (Fig. 13). At
the time of insertion, there should be 45° of elevation Needle Movement Test
angle. Elevation angle is angle between instrument and Once the Veress needle is inside the abdominal cavity,
body of patient. To get an elevation angle of 45° the distal the tip of Veress needle should be free and if surgeon will
Fig. 11: Two Allis forceps is applied over crease of umbilicus. Fig. 12: 2-mm stab wound over inferior crease of umbilicus.
Fig. 13: Veress needle should be held like a dart. Fig. 14: Guard the required length of Veress needle.