
Page 12 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 12
CHAPTER 6: Abdominal Access Techniques 11
The first trocar and cannula inserted is usually 11 mm with Kelly clamp or mosquito forceps (Fig. 26). This will
in diameter. This will accommodate a 10-mm telescope also dilate the obliterated vitellointestinal duct which was
and leave enough space in the cannula for rapid gas demonstrated first time by Scandinavian surgeons so it is
insufflation, if required. called Scandinavian technique.
Steps of Primary Trocar Insertion Introduction of Primary Trocar
Patient Position Surgeon should hold the trocar in proper way. Head of
As for Veress needle insertion, patient should be placed trocar should rest on thenar eminence, middle finger
supine with 10–20° head down. The cephalocaudal should encircle air inlet and index finger should point
relationship between the aortic bifurcation and the toward sharp end (Fig. 27).
umbilicus has been studied radiologically. The umbilicus After holding the trocar properly in hand, full thickness
is often located directly above or cephalad to the aortic of abdominal wall should be lifted by fingers thenar and
bifurcation and is consistently located cephalad to where hypothenar muscles. After creation of pneumoperitoneum,
the left common iliac vein crosses the midline. The aortic lifting of abdominal wall is difficult because it slips. To
bifurcation is located more caudal to the umbilicus in the overcome this, it should be grasped to counter the pressure
Trendelenburg’s position than in the supine position. exerted by the tip of trocar.
Site Angle of Insertion
The same site of Veress needle entry should be used for Initially, angle of insertion for primary trocar should be
primary trocar insertion. Inferior or superior crease perpendicular to abdominal wall but once surgeon feels
of umbilicus can be used in average built patient and giving way sensation, the trocar should be tilted to 60–70°
transumbilical incision can be used in obese patient. angle. Insertion of trocar should be in screwing fashion
Before introduction of trocar, surgeon should confirm in case of pyramidal trocar. In disposable bladed trocar,
pneumoperitoneum. After adequate distention of screwing the trocar should not be done (Fig. 28).
abdominal cavity, the actual pressure should be equal to
the preset pressure and gas flow should be stopped. Confirmation of Entry of Primary Trocar
Before introduction of trocar, the initial 2-mm stab ■ ■Audible click if disposable trocar or safety trocar is
puncture wound of skin for Veress needle should be used.
extended to 11 mm (Fig. 25). It should be remembered ■ ■Whooshing sound if reusable trocar is used (gas passes
that most common cause of forceful entry inside the from the small hole at the tip of pyramidal shaped
abdominal cavity with primary trocar is small skin incision. trocar to the head of trocar).
To avoid inadvertent injury of bowel due to forceful ■ ■Loss of resistance felt both in disposable as well as
uncontrolled entry, the incision of skin should not be <11 reusable trocar.
mm in size. The skin incision for trocar should be smiling Once the trocar entry in abdominal cavity is
in shape (U-shaped) along the crease of umbilicus to get confirmed, cannula is stabilized with left hand and trocar
a better cosmetic value. After giving 11-mm incision with is removed by right hand. After removing trocar, cannula
11 number blades, surgeon should spread fatty tissues is pushed slightly further inside the abdominal cavity to
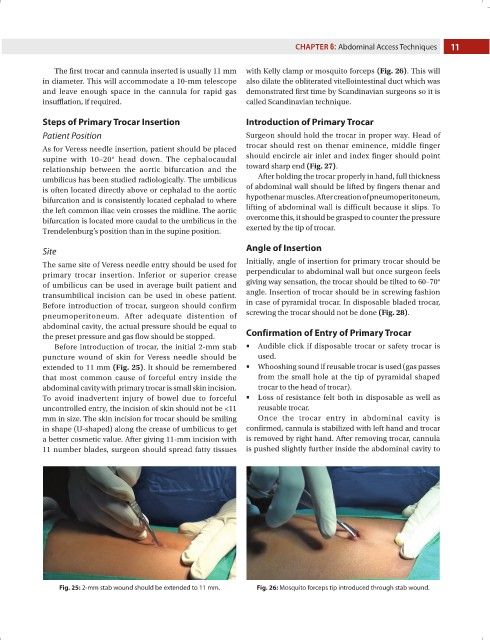
Fig. 25: 2-mm stab wound should be extended to 11 mm. Fig. 26: Mosquito forceps tip introduced through stab wound.