
Page 3 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 3
2 SECTION 1: Essentials of Laparoscopy
where pyramidalis muscle is sometimes found. Therefore, access. Closed technique of access merely by Veress
Veress needle or trocar insertion in these locations rarely needle insertion and creation of pneumoperitoneum is
cause much bleeding. If a defect in the umbilical fascia an easy way of access but it is not possible in some of the
suggests an umbilical hernia or if any midline incision minimal access surgical procedures such as axilloscopy,
scar of previous laparoscopy is found or if any anomalies retroperitoneoscopy, and totally extraperitoneal approach
of the urachus may also exist umbilicus should not be of hernia repair. In general, closed technique by Veress
used for primary access. If an umbilical hernia or urachal needle is possible only if there is a preformed cavity like
anomaly is suspected, alternative access sites may need to abdomen.
be considered. Creation of pneumoperitoneum is one of the most
The colon is attached to the lateral abdominal wall important steps in laparoscopy. The aim is to build up a
along both gutters and puncture laterally for secondary good protective cushion of gas to ensure the safe entry of
trocars should be under video control to avoid visceral trocar and cannula.
injury. When left subcostal site is chosen for access it
should be 2 cm below the costal margin in midclavicular
line called Palmer’s point. The costal margin provides
good resistance as the needle is introduced. When
puncture site lateral to the midline is used, it is prudent
to choose location lateral to the linea semilunaris to avoid
injury of superior and inferior epigastric vessels. In obese
patients, the linea semilunaris may not be visible. In these,
location of inferior artery can be localized by careful
transillumination.
Access to preperitoneal space is gained by penetrating
almost all the layers of abdominal wall except peritoneum.
The open technique of access is preferable in this situation.
After incising the fascia with the scalpel, fingered dissection
is advisable to avoid puncture of peritoneum.
CLOSED ACCESS TECHNIQUE Fig. 2: Veress needle inventor—Janos Veress.
To start any laparoscopic procedure the peritoneal cavity
needs to be accessed, first to establish pneumoperitoneum
and subsequently to place a port for the laparoscope
and add the placement of additional ports for various
laparoscopic instruments. In closed access technique,
pneumoperitoneum is created by Veress needle (named
for Janos Veress) (Fig. 2). The Veress needle was
originally developed by Janos Veress to give patients
with tuberculosis iatrogenic pneumothorax without
damaging the underlying lung parenchyma (Fig. 3).
It has a small-bore (1.8–2.2 mm) needle with a spring-
loaded protective obturator with a side hole that recoils
to cover the end of the needle, allowing entry into a
body cavity without traumatizing the underlying organs Fig. 3: Veress needle.
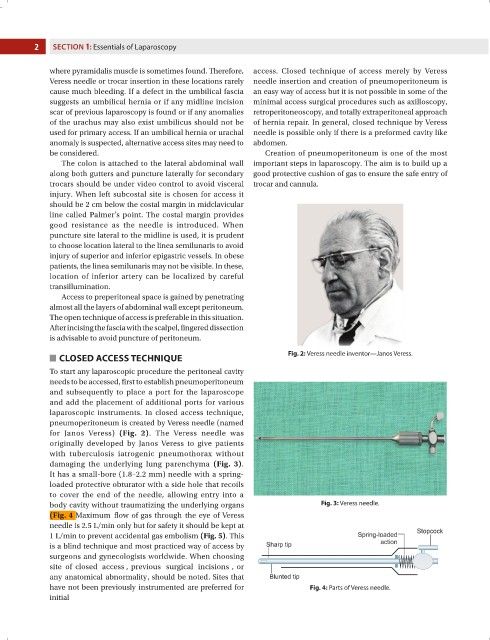
(Fig. 4 Maximum flow of gas through the eye of Veress
needle is 2.5 L/min only but for safety it should be kept at
1 L/min to prevent accidental gas embolism (Fig. 5). This
is a blind technique and most practiced way of access by
surgeons and gynecologists worldwide. When choosing
site of closed access , previous surgical incisions , or
any anatomical abnormality, should be noted. Sites that
have not been previously instrumented are preferred for Fig. 4: Parts of Veress needle.
initial