
Page 11 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 11
10 SECTION 1: Essentials of Laparoscopy
caliber Veress needle can give away CO flow at maximum 5–6 L) to get desired pressure of 12 mm Hg. Whenever
2
2.5 L/min. Once cannula is in place flow rate can be there is less or more amount of gas used to inflate a
increase but when the flow of CO is >10 L/min inside normal abdominal cavity, surgeon should suspect some
2
the abdominal cavity through cannula and there is errors in pneumoperitoneum technique. These errors
leak, there is always a risk of hypothermia and dryness may be leakage or may be preperitoneal space creation or
of intestine. To avoid this hypothermia in all modern extravasation of gas.
microprocessor controlled Laproflattor, there is
an electronic heating system which maintains the PRIMARY TROCAR INSERTION
temperature of CO . Technical errors in the insertion of trocars after creation
2
Total gas used: As soon as 100–200 mL of gas is inside the of pneumoperitoneum are the most common causes
abdominal cavity, surgeon should do percussion of the of injury, resulting from inadequate stabilization of the
right hypochondrium and liver dullness should obliterate abdominal wall, excessive resistance to trocar insertion,
with tympanic sound (Fig. 22). This is the fourth indicator and excessive, misdirected or uncontrolled force applied
of insufflator. Normal size human abdominal cavity needs by the surgeon along the axis of the trocar. It is important to
1.5-L CO to achieve intra-abdominal actual pressure stabilize the abdominal wall by full insufflation, complete
2
of 12 mm Hg. In some big size abdominal cavity and in muscle relaxation, to increase the distance between the
multipara patients, sometimes we need 3 L of CO (rarely anterior abdominal wall and the retroperitoneal vessels
2
and the abdominal organs. It is important to ensure that
the skin incision is of enough length and that the reusable
trocar tip is sharp so that no resistance is offered.
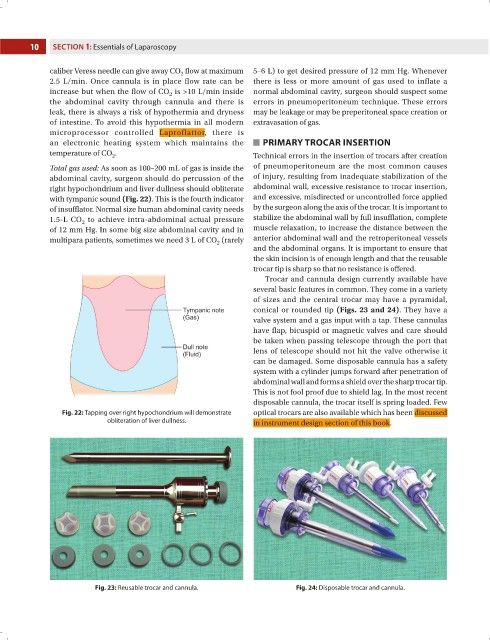
Trocar and cannula design currently available have
several basic features in common. They come in a variety
of sizes and the central trocar may have a pyramidal,
conical or rounded tip (Figs. 23 and 24). They have a
valve system and a gas input with a tap. These cannulas
have flap, bicuspid or magnetic valves and care should
be taken when passing telescope through the port that
lens of telescope should not hit the valve otherwise it
can be damaged. Some disposable cannula has a safety
system with a cylinder jumps forward after penetration of
abdominal wall and forms a shield over the sharp trocar tip.
This is not fool proof due to shield lag. In the most recent
disposable cannula, the trocar itself is spring loaded. Few
Fig. 22: Tapping over right hypochondrium will demonstrate optical trocars are also available which has been discussed
obliteration of liver dullness. in instrument design section of this book.
Fig. 23: Reusable trocar and cannula. Fig. 24: Disposable trocar and cannula.