
Page 2 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 2
6 Abdominal Access Techniques
CHAPTER
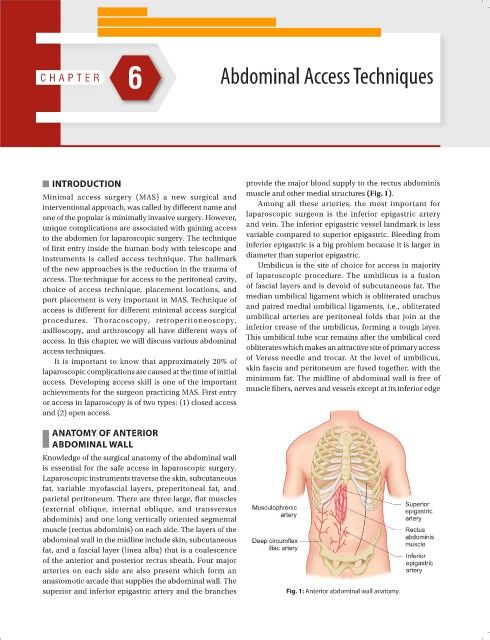
INTRODUCTION provide the major blood supply to the rectus abdominis
muscle and other medial structures (Fig. 1).
Minimal access surgery (MAS) a new surgical and
interventional approach, was called by different name and Among all these arteries, the most important for
one of the popular is minimally invasive surgery. However, laparoscopic surgeon is the inferior epigastric artery
unique complications are associated with gaining access and vein. The inferior epigastric vessel landmark is less
to the abdomen for laparoscopic surgery. The technique variable compared to superior epigastric. Bleeding from
of first entry inside the human body with telescope and inferior epigastric is a big problem because it is larger in
instruments is called access technique. The hallmark diameter than superior epigastric.
of the new approaches is the reduction in the trauma of Umbilicus is the site of choice for access in majority
access. The technique for access to the peritoneal cavity, of laparoscopic procedure. The umbilicus is a fusion
choice of access technique, placement locations, and of fascial layers and is devoid of subcutaneous fat. The
port placement is very important in MAS. Technique of median umbilical ligament which is obliterated urachus
access is different for different minimal access surgical and paired medial umbilical ligaments, i.e., obliterated
procedures. Thoracoscopy, retroperitoneoscopy, umbilical arteries are peritoneal folds that join at the
axilloscopy, and arthroscopy all have different ways of inferior crease of the umbilicus, forming a tough layer.
access. In this chapter, we will discuss various abdominal This umbilical tube scar remains after the umbilical cord
access techniques. obliterates which makes an attractive site of primary access
It is important to know that approximately 20% of of Veress needle and trocar. At the level of umbilicus,
laparoscopic complications are caused at the time of initial skin fascia and peritoneum are fused together, with the
access. Developing access skill is one of the important minimum fat. The midline of abdominal wall is free of
achievements for the surgeon practicing MAS. First entry muscle fibers, nerves and vessels except at its inferior edge
or access in laparoscopy is of two types: (1) closed access
and (2) open access.
ANATOMY OF ANTERIOR
ABDOMINAL WALL
Knowledge of the surgical anatomy of the abdominal wall
is essential for the safe access in laparoscopic surgery.
Laparoscopic instruments traverse the skin, subcutaneous
fat, variable myofascial layers, preperitoneal fat, and
parietal peritoneum. There are three large, flat muscles
(external oblique, internal oblique, and transversus
abdominis) and one long vertically oriented segmental
muscle (rectus abdominis) on each side. The layers of the
abdominal wall in the midline include skin, subcutaneous
fat, and a fascial layer (linea alba) that is a coalescence
of the anterior and posterior rectus sheath. Four major
arteries on each side are also present which form an
anastomotic arcade that supplies the abdominal wall. The
superior and inferior epigastric artery and the branches Fig. 1: Anterior abdominal wall anatomy.