
Page 5 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 5
4 SECTION 1: Essentials of Laparoscopy
comfortably supported by padded obstetric leg holders cases of upper abdominal surgery such as cholecystectomy
or Allen stirrups which minimize the risk of venous called as “American position” .
thrombosis. In these procedures, surgeon needs to use It is not always wise to remain standing in any one
uterine manipulator for proper visualization of female fixed position and surgeon can walk to the other side of
reproductive organs. The assistant seating between the operation table to achieve proper ergonomics. In most
legs of patient will keep on watching the hand movement of the cases at the time of initial access, right-handed
of surgeon on monitor and he should give traction with surgeon should stand on left side of the patient so that he
the handle of uterine monitor in appropriate direction. can hold the Veress needle with right dominant hand. If
If thoracoscopy or retroperitoneoscopy is planned, then surgeon is left-handed, he should stand right to the patient
patient is placed in lateral position (Fig. 7). at the time of access and insert the Veress needle or trocar
with left hand. This helps in inserting Veress needle and
Position of Surgical Team trocar toward pelvis by dominant hand. Once the initial
The laparoscopic surgeon is very much dependent Veress needle and first optical trocar has been introduced
and helpless with eye fixed on monitor. At the time of surgeon should stand opposite to the organ which he
laparoscopic surgery, surgeon is largely depending on wants to operate on. Once all the ports are in position, the
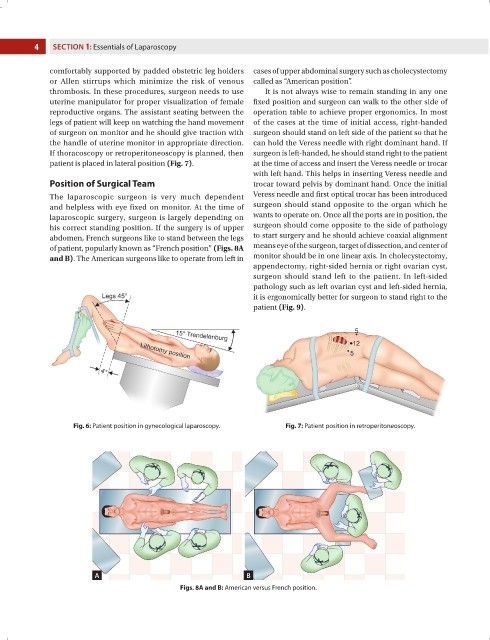
his correct standing position. If the surgery is of upper surgeon should come opposite to the side of pathology
abdomen, French surgeons like to stand between the legs to start surgery and he should achieve coaxial alignment
of patient, popularly known as “French position” (Figs. 8A means eye of the surgeon, target of dissection, and center of
and B). The American surgeons like to operate from left in monitor should be in one linear axis. In cholecystectomy,
appendectomy, right-sided hernia or right ovarian cyst,
surgeon should stand left to the patient. In left-sided
pathology such as left ovarian cyst and left-sided hernia,
it is ergonomically better for surgeon to stand right to the
patient (Fig. 9).
Fig. 6: Patient position in gynecological laparoscopy. Fig. 7: Patient position in retroperitoneoscopy.
A B
Figs. 8A and B: American versus French position.