
Page 13 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 13
12 SECTION 1: Essentials of Laparoscopy
prevent coming cannula in preperitoneal space with vessels. With the help of mosquito forceps, any remaining
movement of abdominal wall with respiration. Once skin fiber is breached, and the subcutaneous fat should
cannula is in place tubing of insufflator is attached again be cleared. Initially, the direction of entry of trocar is
and flow is restarted to refill the CO at preset pressure perpendicular but as soon as the tip of trocar is seen, the
2
(Fig. 29). Telescope is introduced slowly keeping the direction of trocar should be changed toward the free
oblique cut edge down in case of 30° telescope (Fig. 30). At space to prevent any injury of underlying viscera (Fig. 32).
the time of introduction of telescope, it is wise to keep valve
of cannula open to prevent scratch over tip of telescope. Subsequent Ports
Once the telescope is inside, the elevation angle of Subsequent trocars are inserted under direct vision at
the telescope should be 90° with panoramic vision. The locations appropriate for the procedure and to the anatomy
site just below the entry of primary port is examined for of the individual. If the port is on the opposite side of the
any vessel or bowel injury (Fig. 31). Sometime, there patient, it can be introduced same way but if surgeon is not
may be few drops of blood found just below the site of able to bend enough to opposite side, his right index finger
entry but these few drops of blood are trickled blood can be placed over the head of the trocar and left hand
through umbilical wound. If surgeon has any doubt about should guard the shaft of cannula. Alternatively, trocars of
perforation of bowel or injury to vessel, he should evaluate opposite side can be introduced by the assistant (Fig. 33).
this area again after putting other ports. With slow rotatory movement of right hand, first the tip
of trocar should be perpendicular to the skin but as soon
Working Ports as tip of trocar is seen direction of trocar should change
To select the site for secondary port, transillumination toward the anterior abdominal wall. Alternatively, surgeon
with illuminated telescope tip should be done first to can go to another side of the patient and he can introduce
locate avascular area to avoid injury of subcutaneous the trocar in conventional way.
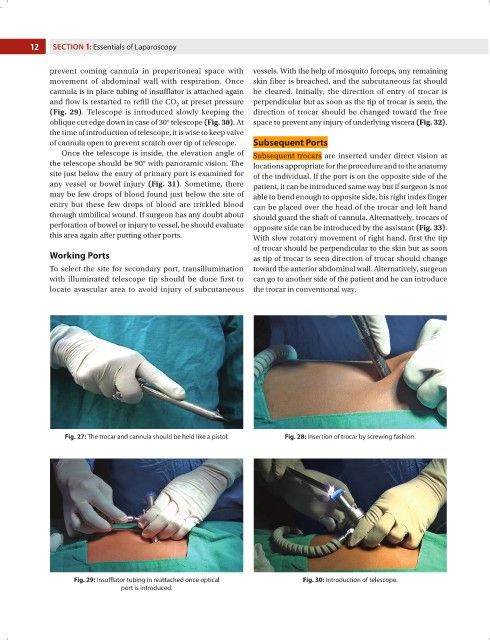
Fig. 27: The trocar and cannula should be held like a pistol. Fig. 28: Insertion of trocar by screwing fashion.
Fig. 29: Insufflator tubing in reattached once optical Fig. 30: Introduction of telescope.
port is introduced.