
Page 21 - WALS Journal
P. 21
Manash Ranjan Sahoo, T Anil Kumar
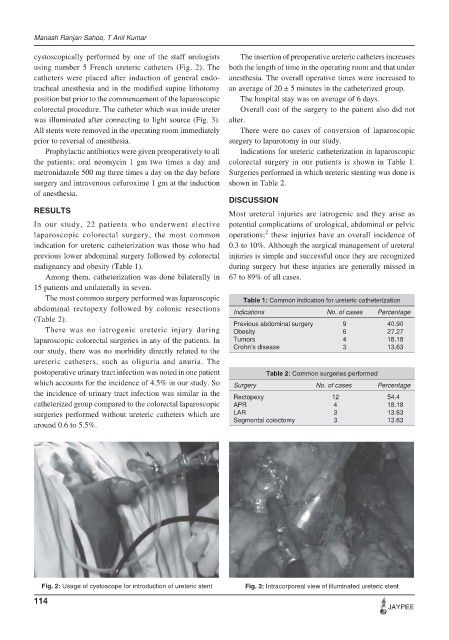
cystoscopically performed by one of the staff urologists The insertion of preoperative ureteric catheters increases
using number 5 French ureteric catheters (Fig. 2). The both the length of time in the operating room and that under
catheters were placed after induction of general endo- anesthesia. The overall operative times were increased to
tracheal anesthesia and in the modified supine lithotomy an average of 20 ± 5 minutes in the catheterized group.
position but prior to the commencement of the laparoscopic The hospital stay was on average of 6 days.
colorectal procedure. The catheter which was inside ureter Overall cost of the surgery to the patient also did not
was illuminated after connecting to light source (Fig. 3). alter.
All stents were removed in the operating room immediately There were no cases of conversion of laparoscopic
prior to reversal of anesthesia. surgery to laparotomy in our study.
Prophylactic antibiotics were given preoperatively to all Indications for ureteric catheterization in laparoscopic
the patients; oral neomycin 1 gm two times a day and colorectal surgery in our patients is shown in Table 1.
metronidazole 500 mg three times a day on the day before Surgeries performed in which ureteric stenting was done is
surgery and intravenous cefuroxime 1 gm at the induction shown in Table 2.
of anesthesia.
DISCUSSION
RESULTS Most ureteral injuries are iatrogenic and they arise as
In our study, 22 patients who underwent elective potential complications of urological, abdominal or pelvic
2
laparoscopic colorectal surgery, the most common operations; these injuries have an overall incidence of
indication for ureteric catheterization was those who had 0.3 to 10%. Although the surgical management of ureteral
previous lower abdominal surgery followed by colorectal injuries is simple and successful once they are recognized
malignancy and obesity (Table 1). during surgery but these injuries are generally missed in
Among them, catheterization was done bilaterally in 67 to 89% of all cases.
15 patients and unilaterally in seven.
The most common surgery performed was laparoscopic Table 1: Common indication for ureteric catheterization
abdominal rectopexy followed by colonic resections
Indications No. of cases Percentage
(Table 2). Previous abdominal surgery 9 40.90
There was no iatrogenic ureteric injury during Obesity 6 27.27
laparoscopic colorectal surgeries in any of the patients. In Tumors 4 18.18
our study, there was no morbidity directly related to the Crohn’s disease 3 13.63
ureteric catheters, such as oliguria and anuria. The
postoperative urinary tract infection was noted in one patient Table 2: Common surgeries performed
which accounts for the incidence of 4.5% in our study. So Surgery No. of cases Percentage
the incidence of urinary tract infection was similar in the Rectopexy 12 54.4
catheterized group compared to the colorectal laparoscopic APR 4 18.18
surgeries performed without ureteric catheters which are LAR 3 13.63
Segmental colectomy 3 13.63
around 0.6 to 5.5%.
Fig. 2: Usage of cystoscope for introduction of ureteric stent Fig. 3: Intracorporeal view of illuminated ureteric stent
114
JAYPEE