
Page 25 - WALS Journal
P. 25
Danish Javed
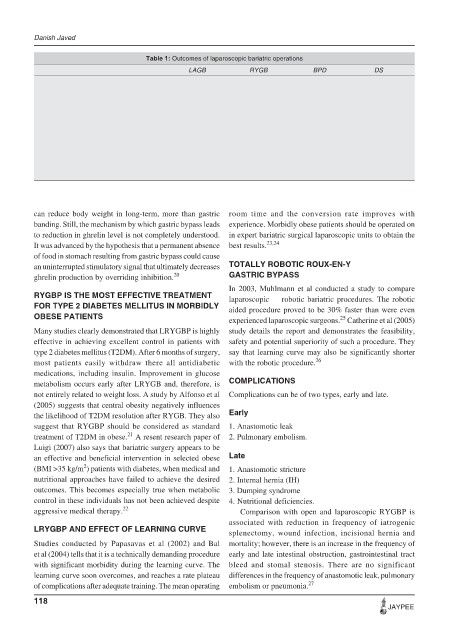
Table 1: Outcomes of laparoscopic bariatric operations
LAGB RYGB BPD DS
Excess weight loss (%) 49-80 60-81 61-78 66-80
Mortality (%) 0-0.2 0-1.0 0.5-1.9 0.4-2.0
Overall morbidity (%) 8.5-25 9-25 22-28 12-20
Nutritional complications (%) Rare 15-25 40-77 39-77
Poor long-term weight loss (%) 10-25 10-15 4-6 3-6
Avg. hospital LOS (days) 1-2 1.9-4 – –
Anastomotic stenosis (%) – 0.1-5 2-13 5-10
Marginal ulcer (%) 2-14 2-14 8-15 0
Hemorrhage (%) 0 0.66 0.2-0.5 0.2-0.5
Wound infection (%) 0 14 0.8 1.0
Leak (%) 1-3 1.3-3 1.2 4.1
Pulmonary embolism (%) 0 0.36-1.2 1-3.6 0.7-1.7
Incisional hernia (%) 0 4.5-14.6 – –
VBG: Vertical banded gastroplasty; RYGB: Roux-en-Y gastric bypass; BPD: Biliopancreatic diversion; DS: Duodenal switch;
LOS: Length of hospital stay
can reduce body weight in long-term, more than gastric room time and the conversion rate improves with
banding. Still, the mechanism by which gastric bypass leads experience. Morbidly obese patients should be operated on
to reduction in ghrelin level is not completely understood. in expert bariatric surgical laparoscopic units to obtain the
It was advanced by the hypothesis that a permanent absence best results. 23,24
of food in stomach resulting from gastric bypass could cause
an uninterrupted stimulatory signal that ultimately decreases TOTALLY ROBOTIC ROUX-EN-Y
ghrelin production by overriding inhibition. 20 GASTRIC BYPASS
In 2003, Muhlmann et al conducted a study to compare
RYGBP IS THE MOST EFFECTIVE TREATMENT laparoscopic vs robotic bariatric procedures. The robotic
FOR TYPE 2 DIABETES MELLITUS IN MORBIDLY aided procedure proved to be 30% faster than were even
OBESE PATIENTS experienced laparoscopic surgeons. Catherine et al (2005)
25
Many studies clearly demonstrated that LRYGBP is highly study details the report and demonstrates the feasibility,
effective in achieving excellent control in patients with safety and potential superiority of such a procedure. They
type 2 diabetes mellitus (T2DM). After 6 months of surgery, say that learning curve may also be significantly shorter
most patients easily withdraw there all antidiabetic with the robotic procedure. 26
medications, including insulin. Improvement in glucose
metabolism occurs early after LRYGB and, therefore, is COMPLICATIONS
not entirely related to weight loss. A study by Alfonso et al Complications can be of two types, early and late.
(2005) suggests that central obesity negatively influences
the likelihood of T2DM resolution after RYGB. They also Early
suggest that RYGBP should be considered as standard 1. Anastomotic leak
21
treatment of T2DM in obese. A resent research paper of 2. Pulmonary embolism.
Luigi (2007) also says that bariatric surgery appears to be
an effective and beneficial intervention in selected obese Late
2
(BMI >35 kg/m ) patients with diabetes, when medical and 1. Anastomotic stricture
nutritional approaches have failed to achieve the desired 2. Internal hernia (IH)
outcomes. This becomes especially true when metabolic 3. Dumping syndrome
control in these individuals has not been achieved despite 4. Nutritional deficiencies.
aggressive medical therapy. 22 Comparison with open and laparoscopic RYGBP is
associated with reduction in frequency of iatrogenic
LRYGBP AND EFFECT OF LEARNING CURVE splenectomy, wound infection, incisional hernia and
Studies conducted by Papasavas et al (2002) and Bal mortality; however, there is an increase in the frequency of
et al (2004) tells that it is a technically demanding procedure early and late intestinal obstruction, gastrointestinal tract
with significant morbidity during the learning curve. The bleed and stomal stenosis. There are no significant
learning curve soon overcomes, and reaches a rate plateau differences in the frequency of anastomotic leak, pulmonary
of complications after adequate training. The mean operating embolism or pneumonia. 27
118
JAYPEE