
Page 29 - World Journal of Laparoscopic Surgery
P. 29
WJOLS
Can Intraperitoneal Tramadol decrease Pain in Patients undergoing Laparoscopic Cholecystectomy in Postoperative Period?
abdominal surgery; American Society for Anesthesiolo- consumption, postoperative hospital course [monitoring of
gists grade III, IV, V or any other significant comorbidity; heart rate (HR), blood pressure (BP), respiratory rate (RR),
and those needing conversion to open cholecystectomy SPO , temperature at 0, 4, 8, 16, and 24 hours, and inci-
2
were excluded from the study. dence of adverse effect (nausea, vomiting, shoulder pain,
After preoxygenation with 100% oxygen for 3 minutes, itching, shivering) at 0, 4, 8, 16, and 24 hours].
induction of anesthesia was achieved with thiopentone Intensity of pain was measured by visual analog
12
sodium (2.5%) 4 to 6 mg/kg intravenous (IV) slowly (till scale (VAS). Patients showing a VAS ≥ 3 or patients who
the abolition of eye lash reflex) along with injection fen- request for analgesia were administered a supplemental
tanyl 1.5 μg/kg IV. Intubation with an appropriate-sized dose of an analgesic (diclofenac sodium; 3 mL, 75 mg).
endotracheal cuffed tube, i.e., facilitated by neuromuscu- Results were reported as mean ± SD. The sample size has
13
lar blocker suxamethonium 1.5 mg/kg IV. been calculated based on the study, where mean pain
Anesthesia was maintained using controlled ventila- score of the normal saline (3.9 ± 2.7) has been consulted.
tion with isoflurane (0.5–1.5%) and nitrous oxide (N O) 66% The sample size per group has been calculated to be 50
2
+ oxygen (O ) 33% using Bain’s circuit. Neuromuscular with 5% level of significance. The 20% reduction in pain at
2
blockade achieved with atracurium besylate. All patients 0 minute has been assumed to be significant reduction.
were given injection metoclopramide 0.5 mg/kg IV This sample size will maintain at least 89% power of the
intraoperatively at the end of procedure. Patients were study. Data was collected and analyzed using Student’s
randomly allocated in double-blind manner using t-test. Epi Info statistical software was used for all analyses.
computer-generated random numbers to one of the two
groups comprising 50 patients each and use of coded RESULTS
syringe which is prepared by anesthesiologist not For this study, 100 patients were recruited. There were no
involved in study. Patients with group I labeled syringe significant differences between two groups according to
(Study group) received intraperitoneal tramadol 100 mg age, sex, and body weight (Table 1).
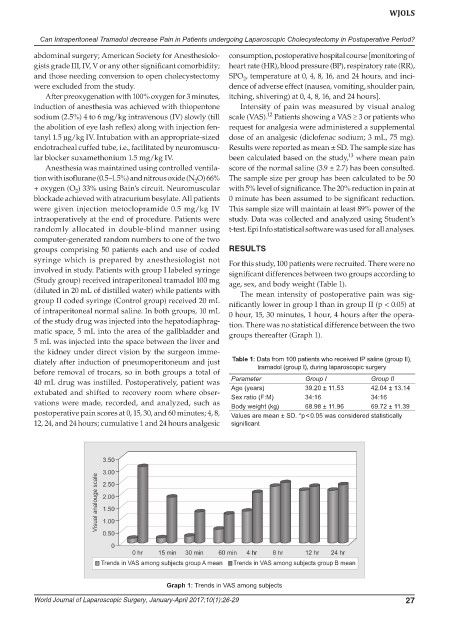
(diluted in 20 mL of distilled water) while patients with The mean intensity of postoperative pain was sig-
group II coded syringe (Control group) received 20 mL nificantly lower in group I than in group II (p < 0.05) at
of intraperitoneal normal saline. In both groups, 10 mL 0 hour, 15, 30 minutes, 1 hour, 4 hours after the opera-
of the study drug was injected into the hepatodiaphrag- tion. There was no statistical difference between the two
matic space, 5 mL into the area of the gallbladder and groups thereafter (Graph 1).
5 mL was injected into the space between the liver and
the kidney under direct vision by the surgeon imme-
diately after induction of pneumoperitoneum and just Table 1: Data from 100 patients who received IP saline (group II),
before removal of trocars, so in both groups a total of tramadol (group I), during laparoscopic surgery
40 mL drug was instilled. Postoperatively, patient was Parameter Group I Group II
extubated and shifted to recovery room where obser- Age (years) 39.20 ± 11.53 42.04 ± 13.14
34:16
Sex ratio (F:M)
34:16
vations were made, recorded, and analyzed, such as Body weight (kg) 68.98 ± 11.96 69.72 ± 11.39
postoperative pain scores at 0, 15, 30, and 60 minutes; 4, 8, Values are mean ± SD. *p < 0.05 was considered statistically
12, 24, and 24 hours; cumulative 1 and 24 hours analgesic significant
Graph 1: Trends in VAS among subjects
World Journal of Laparoscopic Surgery, January-April 2017;10(1):26-29 27