
Page 25 - World Journal of Laparoscopic Surgery
P. 25
WJOLS
Laparoscopic Appendectomy as a Standard of Care for Both Complicated and Uncomplicated Appendicitis in South Africa
The uncertainty about the safety of using LA as a Poor visibility was defined as intraoperative bowel
standard of care in the management of both complicated distension which precludes adequate visualization of
and uncomplicated cases of appendicitis needs clarifica- intraabdominal contents.
tion. The outcomes of this study will suggest if LA as the Successful LA was defined as a patient who under-
standard of care for both complicated and uncomplicated went LA without conversion.
cases of acute appendicitis can be safely practiced.
Statistical Analysis
MATERIALS AND METHODS Means (± SD) are presented for continuous variables and
A retrospective analysis of a prospectively collected frequencies (%) are presented for categorical variables.
data on patients who were offered LA from June 2012 All analyses were performed using SAS version 9.3 (SAS
to October 2015 at DGMAH was done. A database from Institute, Cary, NC).
the Department of General Surgery at Sefako Makgatho RESULTS
Health Sciences University (SMU) was used to retrieve
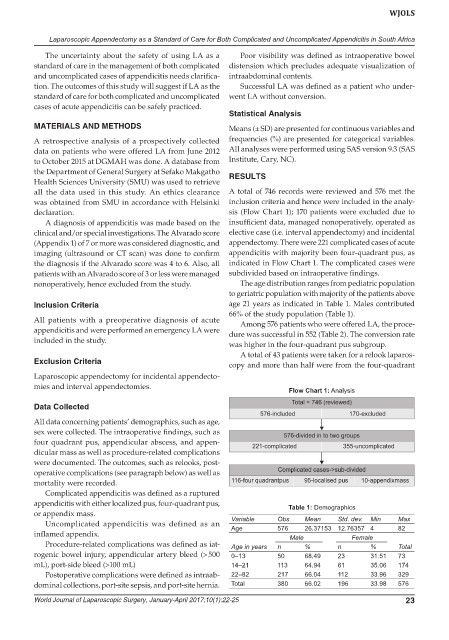
all the data used in this study. An ethics clearance A total of 746 records were reviewed and 576 met the
was obtained from SMU in accordance with Helsinki inclusion criteria and hence were included in the analy-
declaration. sis (Flow Chart 1); 170 patients were excluded due to
A diagnosis of appendicitis was made based on the insufficient data, managed nonoperatively, operated as
clinical and/or special investigations. The Alvarado score elective case (i.e. interval appendectomy) and incidental
(Appendix 1) of 7 or more was considered diagnostic, and appendectomy. There were 221 complicated cases of acute
imaging (ultrasound or CT scan) was done to confirm appendicitis with majority been four-quadrant pus, as
the diagnosis if the Alvarado score was 4 to 6. Also, all indicated in Flow Chart 1. The complicated cases were
patients with an Alvarado score of 3 or less were managed subdivided based on intraoperative findings.
nonoperatively, hence excluded from the study. The age distribution ranges from pediatric population
to geriatric population with majority of the patients above
Inclusion Criteria age 21 years as indicated in Table 1. Males contributed
66% of the study population (Table 1).
All patients with a preoperative diagnosis of acute Among 576 patients who were offered LA, the proce-
appendicitis and were performed an emergency LA were dure was successful in 552 (Table 2). The conversion rate
included in the study.
was higher in the four-quadrant pus subgroup.
A total of 43 patients were taken for a relook laparos-
Exclusion Criteria copy and more than half were from the four-quadrant
Laparoscopic appendectomy for incidental appendecto-
mies and interval appendectomies.
Flow Chart 1: Analysis
Data Collected
All data concerning patients’ demographics, such as age,
sex were collected. The intraoperative findings, such as
four quadrant pus, appendicular abscess, and appen-
dicular mass as well as procedure-related complications
were documented. The outcomes, such as relooks, post-
operative complications (see paragraph below) as well as
mortality were recorded.
Complicated appendicitis was defined as a ruptured
appendicitis with either localized pus, four-quadrant pus, Table 1: Demographics
or appendix mass.
Uncomplicated appendicitis was defined as an Variable Obs. Mean Std. dev. Min Max
576
Age
82
26.37153 12.76357 4
inflamed appendix. Male Female
Procedure-related complications was defined as iat- Age in years n % n % Total
rogenic bowel injury, appendicular artery bleed (> 500 0–13 50 68.49 23 31.51 73
mL), port-side bleed (>100 mL) 14–21 113 64.94 61 35.06 174
Postoperative complications were defined as intraab- 22–82 217 66.04 112 33.96 329
dominal collections, port-site sepsis, and port-site hernia. Total 380 66.02 196 33.98 576
World Journal of Laparoscopic Surgery, January-April 2017;10(1):22-25 23