
Page 22 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 22
CHAPTER 6: Abdominal Access Techniques 21
port wound, the chances of port-site hernia and adhesion properly to prevent any future possibility of hernia. The
are much higher in this case. It is a good practice to insert rectus sheath is only necessary to suture with Vicryl.
some blunt instrument or telescope inside the abdomen Only one stitch is required in middle which will convert
while removing the last cannula out over that instrument, 10 mm wound into 5 mm. The 5 mm port wounds are not
to prevent inadvertent entrapment of omentum or bowel necessary to repair (Figs. 56A to D).
(Figs. 55A and B). Various types of port closure instruments are available.
The suture passer is a convenient instrument for port
PORT CLOSURE TECHNIQUES closure, it is used to pass the thread on the side of cannula
The access technique will result in breach in continuity of and then it is tied externally (Figs. 57A and B). For port
abdominal wall which need to be repaired at the end of closure, specially designed port closure instruments are
surgery. All the 10 mm or >10 mm port should be repaired also available commercially, such as port closure needle
and aneurism needle. After closing the rectus sheath, the
skin can be closed by intradermal, skin stapler or by any of
the surgical skin glues available (Fig. 58).
Gasless Laparoscopic Surgery
Conventional laparoscopic surgery requires
pneumoperitoneum to elevate the abdominal wall
for proper exposure. A continuous insufflation of a
A B noncombustible gas in a sealed environment is essential
part of MAS. Many undesirable physiological side effects
have been observed with CO pneumoperitoneum.
2
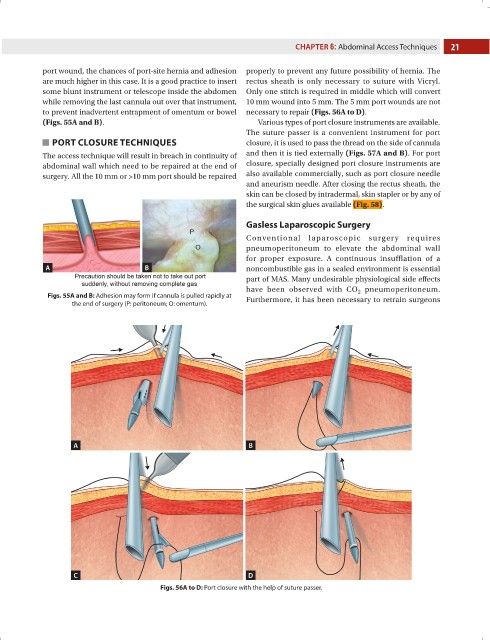
Figs. 55A and B: Adhesion may form if cannula is pulled rapidly at Furthermore, it has been necessary to retrain surgeons
the end of surgery (P: peritoneum; O: omentum).
A B
C D
Figs. 56A to D: Port closure with the help of suture passer.