
Page 19 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 19
18 SECTION 1: Essentials of Laparoscopy
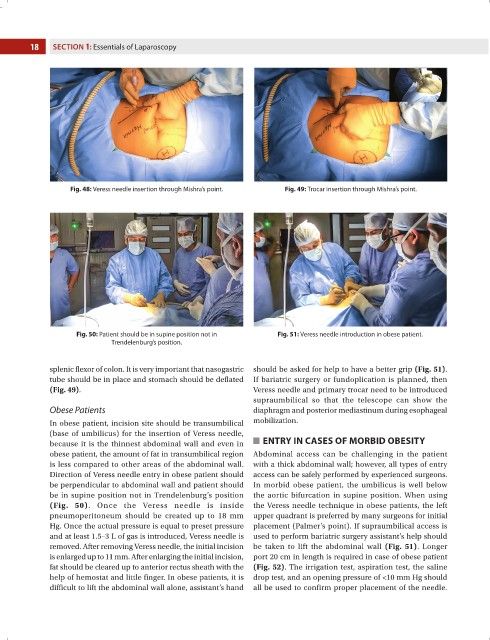
Fig. 48: Veress needle insertion through Mishra’s point. Fig. 49: Trocar insertion through Mishra’s point.
Fig. 50: Patient should be in supine position not in Fig. 51: Veress needle introduction in obese patient.
Trendelenburg’s position.
splenic flexor of colon. It is very important that nasogastric should be asked for help to have a better grip (Fig. 51).
tube should be in place and stomach should be deflated If bariatric surgery or fundoplication is planned, then
(Fig. 49). Veress needle and primary trocar need to be introduced
supraumbilical so that the telescope can show the
Obese Patients diaphragm and posterior mediastinum during esophageal
In obese patient, incision site should be transumbilical mobilization.
(base of umbilicus) for the insertion of Veress needle,
because it is the thinnest abdominal wall and even in ENTRY IN CASES OF MORBID OBESITY
obese patient, the amount of fat in transumbilical region Abdominal access can be challenging in the patient
is less compared to other areas of the abdominal wall. with a thick abdominal wall; however, all types of entry
Direction of Veress needle entry in obese patient should access can be safely performed by experienced surgeons.
be perpendicular to abdominal wall and patient should In morbid obese patient, the umbilicus is well below
be in supine position not in Trendelenburg’s position the aortic bifurcation in supine position. When using
(Fig. 50). Once the Veress needle is inside the Veress needle technique in obese patients, the left
pneumoperitoneum should be created up to 18 mm upper quadrant is preferred by many surgeons for initial
Hg. Once the actual pressure is equal to preset pressure placement (Palmer’s point). If supraumbilical access is
and at least 1.5–3 L of gas is introduced, Veress needle is used to perform bariatric surgery assistant’s help should
removed. After removing Veress needle, the initial incision be taken to lift the abdominal wall (Fig. 51). Longer
is enlarged up to 11 mm. After enlarging the initial incision, port 20 cm in length is required in case of obese patient
fat should be cleared up to anterior rectus sheath with the (Fig. 52). The irrigation test, aspiration test, the saline
help of hemostat and little finger. In obese patients, it is drop test, and an opening pressure of <10 mm Hg should
difficult to lift the abdominal wall alone, assistant’s hand all be used to confirm proper placement of the needle.