
Page 24 - Textbook of Practical Laparoscopic Surgery by Dr. R. K. Mishra
P. 24
CHAPTER 6: Abdominal Access Techniques 23
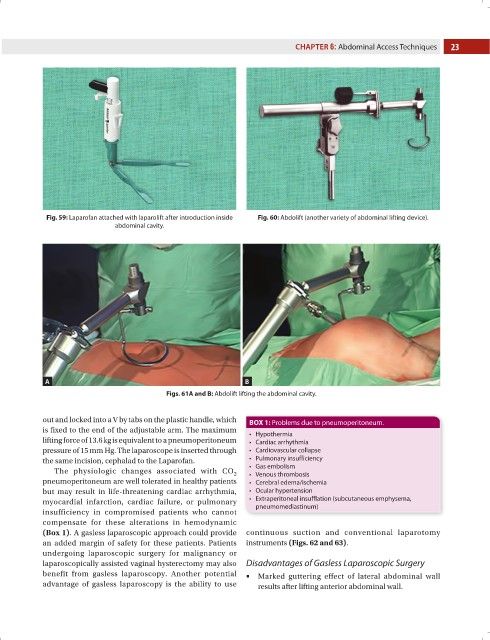
Fig. 59: Laparofan attached with laparolift after introduction inside Fig. 60: Abdolift (another variety of abdominal lifting device).
abdominal cavity.
A B
Figs. 61A and B: Abdolift lifting the abdominal cavity.
out and locked into a V by tabs on the plastic handle, which BOX 1: Problems due to pneumoperitoneum.
is fixed to the end of the adjustable arm. The maximum • Hypothermia
lifting force of 13.6 kg is equivalent to a pneumoperitoneum • Cardiac arrhythmia
pressure of 15 mm Hg. The laparoscope is inserted through • Cardiovascular collapse
the same incision, cephalad to the Laparofan. • Pulmonary insufficiency
The physiologic changes associated with CO • Gas embolism
• Venous thrombosis
2
pneumoperitoneum are well tolerated in healthy patients • Cerebral edema/ischemia
but may result in life-threatening cardiac arrhythmia, • Ocular hypertension
myocardial infarction, cardiac failure, or pulmonary • Extraperitoneal insufflation (subcutaneous emphysema,
pneumomediastinum)
insufficiency in compromised patients who cannot
compensate for these alterations in hemodynamic
(Box 1). A gasless laparoscopic approach could provide continuous suction and conventional laparotomy
an added margin of safety for these patients. Patients instruments (Figs. 62 and 63).
undergoing laparoscopic surgery for malignancy or
laparoscopically assisted vaginal hysterectomy may also Disadvantages of Gasless Laparoscopic Surgery
benefit from gasless laparoscopy. Another potential ■ ■Marked guttering effect of lateral abdominal wall
advantage of gasless laparoscopy is the ability to use results after lifting anterior abdominal wall.