
Page 18 - WJOLS - Journal of Laparoscopic Surgery
P. 18
WJOLS
Can Robotic Gastrectomy be considered as Gold Standard for Upcoming Surgeons?
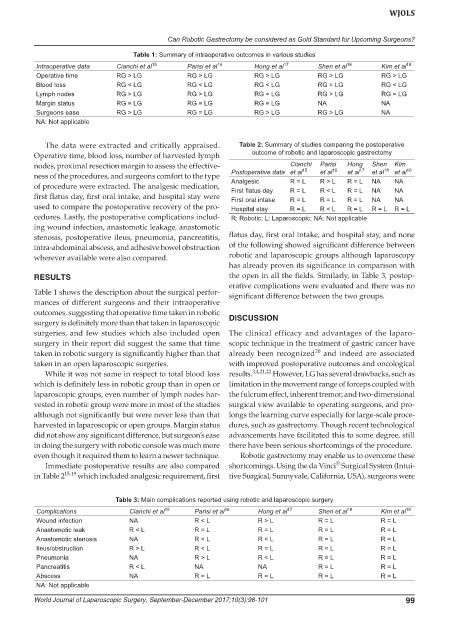
Table 1: Summary of intraoperative outcomes in various studies
Intraoperative data Cianchi et al 15 Parisi et al 16 Hong et al 17 Shen et al 18 Kim et al 19
Operative time RG > LG RG > LG RG > LG RG > LG RG > LG
Blood loss RG < LG RG < LG RG < LG RG = LG RG < LG
Lymph nodes RG > LG RG > LG RG = LG RG > LG RG = LG
Margin status RG = LG RG = LG RG = LG NA NA
Surgeons ease RG > LG RG = LG RG > LG RG > LG NA
NA: Not applicable
The data were extracted and critically appraised. Table 2: Summary of studies comparing the postoperative
Operative time, blood loss, number of harvested lymph outcome of robotic and laparoscopic gastrectomy
nodes, proximal resection margin to assess the effective- Cianchi Parisi Hong Shen Kim 19
17
18
15
16
ness of the procedures, and surgeons comfort to the type Postoperative data et al et al et al et al et al
of procedure were extracted. The analgesic medication, Analgesic R = L R > L R = L NA NA
NA
R < L
NA
R = L
First flatus day
R = L
first flatus day, first oral intake, and hospital stay were First oral intake R = L R = L R = L NA NA
used to compare the postoperative recovery of the pro- Hospital stay R = L R < L R = L R = L R = L
cedures. Lastly, the postoperative complications includ- R: Robotic; L: Laparoscopic; NA: Not applicable
ing wound infection, anastomotic leakage, anastomotic
stenosis, postoperative ileus, pneumonia, pancreatitis, flatus day, first oral intake, and hospital stay, and none
intra-abdominal abscess, and adhesive bowel obstruction of the following showed significant difference between
wherever available were also compared. robotic and laparoscopic groups although laparoscopy
has already proven its significance in comparison with
RESULTS the open in all the fields. Similarly, in Table 3, postop-
erative complications were evaluated and there was no
Table 1 shows the description about the surgical perfor- significant difference between the two groups.
mances of different surgeons and their intraoperative
outcomes, suggesting that operative time taken in robotic
surgery is definitely more than that taken in laparoscopic DISCUSSION
surgeries, and few studies which also included open The clinical efficacy and advantages of the laparo-
surgery in their report did suggest the same that time scopic technique in the treatment of gastric cancer have
20
taken in robotic surgery is significantly higher than that already been recognized and indeed are associated
taken in an open laparoscopic surgeries. with improved postoperative outcomes and oncological
While it was not same in respect to total blood loss results. 3,4,21,22 However, LG has several drawbacks, such as
which is definitely less in robotic group than in open or limitation in the movement range of forceps coupled with
laparoscopic groups, even number of lymph nodes har- the fulcrum effect, inherent tremor, and two-dimensional
vested in robotic group were more in most of the studies surgical view available to operating surgeons, and pro-
although not significantly but were never less than that longs the learning curve especially for large-scale proce-
harvested in laparoscopic or open groups. Margin status dures, such as gastrectomy. Though recent technological
did not show any significant difference, but surgeon’s ease advancements have facilitated this to some degree, still
in doing the surgery with robotic console was much more there have been serious shortcomings of the procedure.
even though it required them to learn a newer technique. Robotic gastrectomy may enable us to overcome these
®
Immediate postoperative results are also compared shortcomings. Using the da Vinci Surgical System (Intui-
in Table 2 15-19 which included analgesic requirement, first tive Surgical, Sunnyvale, California, USA), surgeons were
Table 3: Main complications reported using robotic and laparoscopic surgery
Complications Cianchi et al 15 Parisi et al 16 Hong et al 17 Shen et al 18 Kim et al 19
Wound infection NA R < L R > L R = L R = L
Anastomotic leak R < L R = L R = L R = L R = L
Anastomotic stenosis NA R < L R < L R = L R = L
Ileus/obstruction R > L R < L R = L R = L R = L
Pneumonia NA R > L R < L R = L R = L
Pancreatitis R < L NA NA R = L R = L
Abscess NA R = L R = L R = L R = L
NA: Not applicable
World Journal of Laparoscopic Surgery, September-December 2017;10(3):98-101 99