
Page 13 - Journal of Laparoscopic Surgery
P. 13
WJOLS
Two Port Laparoscopic Cholecystectomy—An Initial Experience of 25 Cases with a New Technique
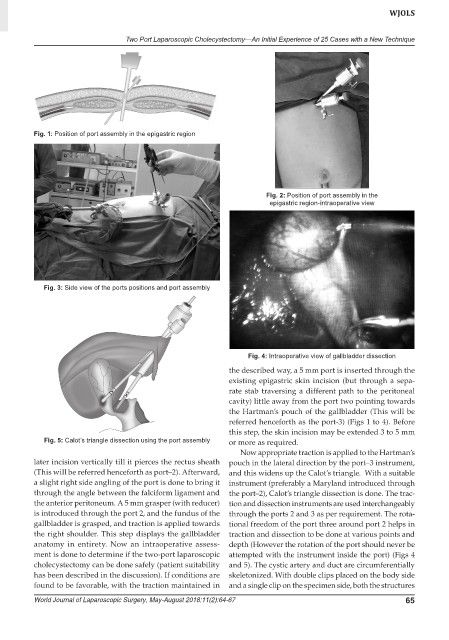
Fig. 1: Position of port assembly in the epigastric region
Fig. 2: Position of port assembly in the
epigastric region-intraoperative view
Fig. 3: Side view of the ports positions and port assembly
Fig. 4: Intraoperative view of gallbladder dissection
the described way, a 5 mm port is inserted through the
existing epigastric skin incision (but through a sepa-
rate stab traversing a different path to the peritoneal
cavity) little away from the port two pointing towards
the Hartman’s pouch of the gallbladder (This will be
referred henceforth as the port-3) (Figs 1 to 4). Before
this step, the skin incision may be extended 3 to 5 mm
Fig. 5: Calot’s triangle dissection using the port assembly or more as required.
Now appropriate traction is applied to the Hartman’s
later incision vertically till it pierces the rectus sheath pouch in the lateral direction by the port–3 instrument,
(This will be referred henceforth as port–2). Afterward, and this widens up the Calot’s triangle. With a suitable
a slight right side angling of the port is done to bring it instrument (preferably a Maryland introduced through
through the angle between the falciform ligament and the port–2), Calot’s triangle dissection is done. The trac-
the anterior peritoneum. A 5 mm grasper (with reducer) tion and dissection instruments are used interchangeably
is introduced through the port 2, and the fundus of the through the ports 2 and 3 as per requirement. The rota-
gallbladder is grasped, and traction is applied towards tional freedom of the port three around port 2 helps in
the right shoulder. This step displays the gallbladder traction and dissection to be done at various points and
anatomy in entirety. Now an intraoperative assess- depth (However the rotation of the port should never be
ment is done to determine if the two-port laparoscopic attempted with the instrument inside the port) (Figs 4
cholecystectomy can be done safely (patient suitability and 5). The cystic artery and duct are circumferentially
has been described in the discussion). If conditions are skeletonized. With double clips placed on the body side
found to be favorable, with the traction maintained in and a single clip on the specimen side, both the structures
World Journal of Laparoscopic Surgery, May-August 2018;11(2):64-67 65