
Page 19 - World Journal of Laparoscopic Surgery
P. 19
Safety and Feasibility of Sleeve Gastrectomy with Loop Duodenal Switch
Institutional ethics committee approval was obtained and detailed
written informed consent was taken from all the participants in this
study. Our study complied with the ethical norms proposed by the
Helsinki declaration for research involving humans.
Technique
Four ports were used in all the patients. Devascularization of greater
curvature was performed starting opposite to angular incisure.
Dissection was continued up to 5 cm beyond the pylorus and
behind the first part of the duodenum until the gastroduodenal
artery was identified (Fig. 2). The lesser omental layer over the
caudate lobe was divided from behind the stomach to create a
window. The right gastric artery (RGA) was divided at its origin
using a vessel sealer. This step was a modification compared to
7,8
the classical SADI-S described by Sánchez-Pernaute et al. This
step ensured free mobility of gastric sleeve, pylorus, and the
first part of the duodenum as a single unit after the duodenal
9
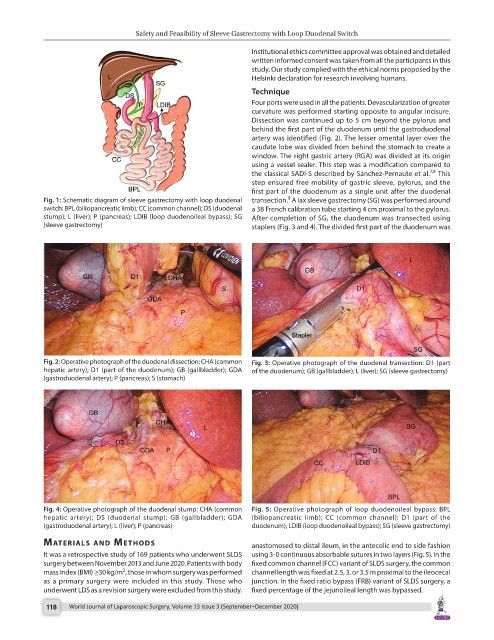
Fig. 1: Schematic diagram of sleeve gastrectomy with loop duodenal transection. A lax sleeve gastrectomy (SG) was performed around
switch: BPL (biliopancreatic limb); CC (common channel); DS (duodenal a 38 French calibration tube starting 4 cm proximal to the pylorus.
stump); L (liver); P (pancreas); LDIB (loop duodenoileal bypass); SG After completion of SG, the duodenum was transected using
(sleeve gastrectomy) staplers (Fig. 3 and 4). The divided first part of the duodenum was
Fig. 2: Operative photograph of the duodenal dissection: CHA (common Fig. 3: Operative photograph of the duodenal transection: D1 (part
hepatic artery); D1 (part of the duodenum); GB (gallbladder); GDA of the duodenum); GB (gallbladder); L (liver); SG (sleeve gastrectomy)
(gastroduodenal artery); P (pancreas); S (stomach)
Fig. 4: Operative photograph of the duodenal stump: CHA (common Fig. 5: Operative photograph of loop duodenoileal bypass: BPL
hepatic artery); DS (duodenal stump); GB (gallbladder); GDA (biliopancreatic limb); CC (common channel); D1 (part of the
(gastroduodenal artery); L (liver); P (pancreas) duodenum); LDIB (loop duodenoileal bypass); SG (sleeve gastrectomy)
MAterIAls And Methods anastomosed to distal ileum, in the antecolic end to side fashion
It was a retrospective study of 169 patients who underwent SLDS using 3-0 continuous absorbable sutures in two layers (Fig. 5). In the
surgery between November 2013 and June 2020. Patients with body fixed common channel (FCC) variant of SLDS surgery, the common
2
mass index (BMI) ≥30 kg/m , those in whom surgery was performed channel length was fixed at 2.5, 3, or 3.5 m proximal to the ileocecal
as a primary surgery were included in this study. Those who junction. In the fixed ratio bypass (FRB) variant of SLDS surgery, a
underwent LDS as a revision surgery were excluded from this study. fixed percentage of the jejunoileal length was bypassed.
118 World Journal of Laparoscopic Surgery, Volume 13 Issue 3 (September–December 2020)