
Page 9 - World Journal of Laparoscopic Surgery
P. 9
Case Report Related to Laparoscopic Cholecystectomy
PATHOLOGIC FINDINGS
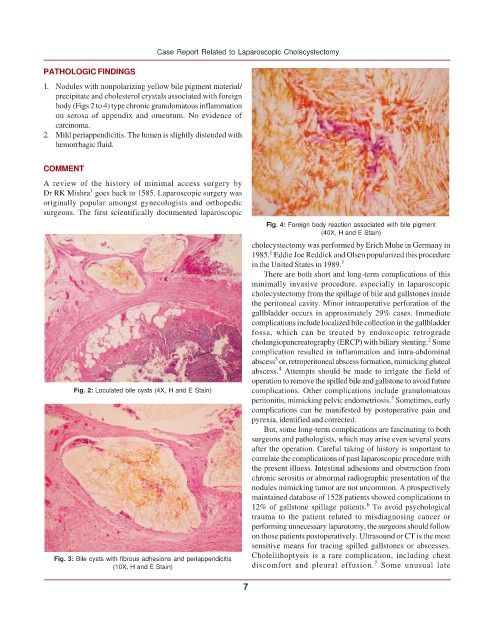
1. Nodules with nonpolarizing yellow bile pigment material/
precipitate and cholesterol crystals associated with foreign
body (Figs 2 to 4) type chronic granulomatous inflammation
on serosa of appendix and omentum. No evidence of
carcinoma.
2. Mild periappendicitis. The lumen is slightly distended with
hemorrhagic fluid.
COMMENT
A review of the history of minimal access surgery by
1
Dr RK Mishra goes back to 1585. Laparoscopic surgery was
originally popular amongst gynecologists and orthopedic
surgeons. The first scientifically documented laparoscopic
Fig. 4: Foreign body reaction associated with bile pigment
(40X, H and E Stain)
cholecystectomy was performed by Erich Muhe in Germany in
1
1985. Eddie Joe Reddick and Olsen popularized this procedure
in the United States in 1989. 1
There are both short and long-term complications of this
minimally invasive procedure, especially in laparoscopic
cholecystectomy from the spillage of bile and gallstones inside
the peritoneal cavity. Minor intraoperative perforation of the
gallbladder occurs in approximately 29% cases. Immediate
complications include localized bile collection in the gallbladder
fossa, which can be treated by endoscopic retrograde
2
cholangiopancreatography (ERCP) with biliary stenting. Some
complication resulted in inflammation and intra-abdominal
3
abscess or, retroperitoneal abscess formation, mimicking gluteal
4
abscess. Attempts should be made to irrigate the field of
operation to remove the spilled bile and gallstone to avoid future
Fig. 2: Loculated bile cysts (4X, H and E Stain) complications. Other complications include granulomatous
5
peritonitis, mimicking pelvic endometriosis. Sometimes, early
complications can be manifested by postoperative pain and
pyrexia, identified and corrected.
But, some long-term complications are fascinating to both
surgeons and pathologists, which may arise even several years
after the operation. Careful taking of history is important to
correlate the complications of past laparoscopic procedure with
the present illness. Intestinal adhesions and obstruction from
chronic serositis or abnormal radiographic presentation of the
nodules mimicking tumor are not uncommon. A prospectively
maintained database of 1528 patients showed complications in
6
12% of gallstone spillage patients. To avoid psychological
trauma to the patient related to misdiagnosing cancer or
performing unnecessary laparotomy, the surgeons should follow
on those patients postoperatively. Ultrasound or CT is the most
sensitive means for tracing spilled gallstones or abscesses.
Cholelithoptysis is a rare complication, including chest
Fig. 3: Bile cysts with fibrous adhesions and periappendicitis 7
(10X, H and E Stain) discomfort and pleural effusion. Some unusual late
7