
Page 8 - World Journal of Laparoscopic Surgery
P. 8
Anup Hazra et al
World Journal of Laparoscopic Surgery, January-April 2008;1(1):6-8
Case Report Related to
Laparoscopic Cholecystectomy
Anup Hazra, Richard Siderits, Archan Hazra, Janusz Godyn
Department of Pathology and Laboratory Medicine, UMDNJ-RWJ Medical School and RWJ University Hospital at Hamilton
Hamilton, NJ 08690, USA
Correspondence: Anup Hazra
Associate Professor of Pathology and Laboratory Medicine, RWJ Medical School
Vice Chairman and Director of Laboratories, Department of Pathology and Laboratory Medicine
RWJ University Hospital at Hamilton, 1 Hamilton Health Place, Hamilton, NJ 08690
609-584-6569 (p), 609-584-6439 (f), ahazra@rwjuhh.edu, hazraan@yahoo.com
INTRODUCTION Preliminary impression was to rule out acute appendicitis,
ectopic pregnancy or urinary tract infection.
Post laparoscopic cholecystectomy bile spillage, presented
clinically as acute appendicitis, mimicking intraoperatively MATERIALS AND METHODS
peritoneal carcinomatosis.
Laparoscopic cholecystectomy is a highly popular, The urinalysis shows no pathologic findings and urine cultures
minimally invasive surgery, which outweighs the standard were negative. The patient was admitted for diagnostic
“open” surgery for gallbladder operation. However, there are laparoscopy and probable laparoscopic appendectomy. During
some short-term and long-term complications as a result of the procedure, the surgeon noted multiple small yellow nodules
intraoperative spillage of bile and gallstones during laparoscopic studded on the omentum, serosa of the appendix, and pelvic
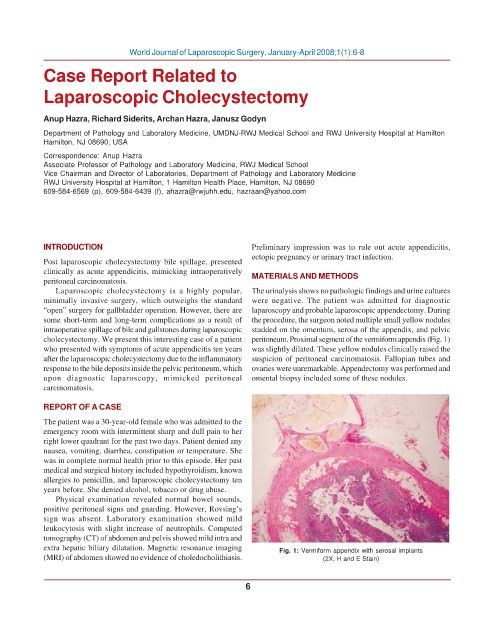
cholecystectomy. We present this interesting case of a patient peritoneum. Proximal segment of the vermiform appendix (Fig. 1)
who presented with symptoms of acute appendicitis ten years was slightly dilated. These yellow nodules clinically raised the
after the laparoscopic cholecystectomy due to the inflammatory suspicion of peritoneal carcinomatosis. Fallopian tubes and
response to the bile deposits inside the pelvic peritoneum, which ovaries were unremarkable. Appendectomy was performed and
upon diagnostic laparoscopy, mimicked peritoneal omental biopsy included some of these nodules.
carcinomatosis.
REPORT OF A CASE
The patient was a 30-year-old female who was admitted to the
emergency room with intermittent sharp and dull pain to her
right lower quadrant for the past two days. Patient denied any
nausea, vomiting, diarrhea, constipation or temperature. She
was in complete normal health prior to this episode. Her past
medical and surgical history included hypothyroidism, known
allergies to penicillin, and laparoscopic cholecystectomy ten
years before. She denied alcohol, tobacco or drug abuse.
Physical examination revealed normal bowel sounds,
positive peritoneal signs and guarding. However, Rovsing’s
sign was absent. Laboratory examination showed mild
leukocytosis with slight increase of neutrophils. Computed
tomography (CT) of abdomen and pelvis showed mild intra and
extra hepatic biliary dilatation. Magnetic resonance imaging Fig. 1: Vermiform appendix with serosal implants
(MRI) of abdomen showed no evidence of choledocholithiasis. (2X, H and E Stain)
6