
Page 16 - WJOLS - Laparoscopic Journal
P. 16
Recent Advances in Laparoscopic Hysterectomy: Journey from Multiple Incision to Single Incision Hysterectomy
EQUIPMENT FOR SILS
The specialized instruments used in SILS are available with
following configuration:
• SILS device from Covidien
• Gel Point system from applied medical
• R-Port and TriPort from advanced surgical concepts
• Uni-X from Pnavel.
Hand Instruments for SILS comes in Two
Configurations
• Standard laparoscopic instruments
• Articulating instruments.
DIFFERENCE IN SILS OPERATIVE TECHNIQUE
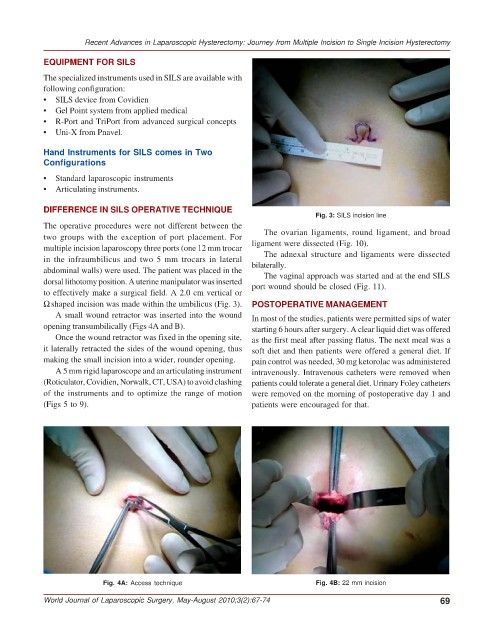
Fig. 3: SILS incision line
The operative procedures were not different between the
two groups with the exception of port placement. For The ovarian ligaments, round ligament, and broad
multiple incision laparoscopy three ports (one 12 mm trocar ligament were dissected (Fig. 10).
The adnexal structure and ligaments were dissected
in the infraumbilicus and two 5 mm trocars in lateral bilaterally.
abdominal walls) were used. The patient was placed in the The vaginal approach was started and at the end SILS
dorsal lithotomy position. A uterine manipulator was inserted port wound should be closed (Fig. 11).
to effectively make a surgical field. A 2.0 cm vertical or
Ω shaped incision was made within the umbilicus (Fig. 3). POSTOPERATIVE MANAGEMENT
A small wound retractor was inserted into the wound In most of the studies, patients were permitted sips of water
opening transumbilically (Figs 4A and B). starting 6 hours after surgery. A clear liquid diet was offered
Once the wound retractor was fixed in the opening site, as the first meal after passing flatus. The next meal was a
it laterally retracted the sides of the wound opening, thus soft diet and then patients were offered a general diet. If
making the small incision into a wider, rounder opening. pain control was needed, 30 mg ketorolac was administered
A 5 mm rigid laparoscope and an articulating instrument intravenously. Intravenous catheters were removed when
(Roticulator, Covidien, Norwalk, CT, USA) to avoid clashing patients could tolerate a general diet. Urinary Foley catheters
of the instruments and to optimize the range of motion were removed on the morning of postoperative day 1 and
(Figs 5 to 9). patients were encouraged for that.
Fig. 4A: Access technique Fig. 4B: 22 mm incision
World Journal of Laparoscopic Surgery, May-August 2010;3(2):67-74 69