
Page 11 - WJOLS - Laparoscopic Journal
P. 11
WJOLS
ORIGINAL ARTICLE Laparoscopic Cholecystectomy in Situs Inversus Totalis
Laparoscopic Cholecystectomy in Situs
Inversus Totalis
Sardar H Arif
Department of Surgery, Duhok Medical College, Azadi Teaching Hospital, Duhok, Kurdistan Region, Iraq
Abstract
A 42-year-old female known case of situs inversus presented with several attacks of epigastric pain. Abdominal ultrasound confirmed the
diagnosis of gallstone, as well as situs inversus, laparoscopic cholecystectomy was performed safely, the operation done by left handed
surgeon.
Keywords: Laparoscopic cholecystectomy, situs inversus.
INTRODUCTION
Situs inversus totalis is first described in 1600, situs inversus
totalis is a rare congenital anomaly with an autosomal
recessive genetic pattern of inheritance, which is usually
asymptomatic through adulthood. In the absence of rare
1
cardiac anomalies, life-expectancy is normal. It may be
partial, where the transposition is confined to either the
abdominal or the thoracic viscera, or complete, i.e. involving
2
both the cavities. While acute cholecystitis is one of the
most common diagnosis requiring surgical management, it
can be difficult to correctly diagnose in a patient with situs
inversus. 3
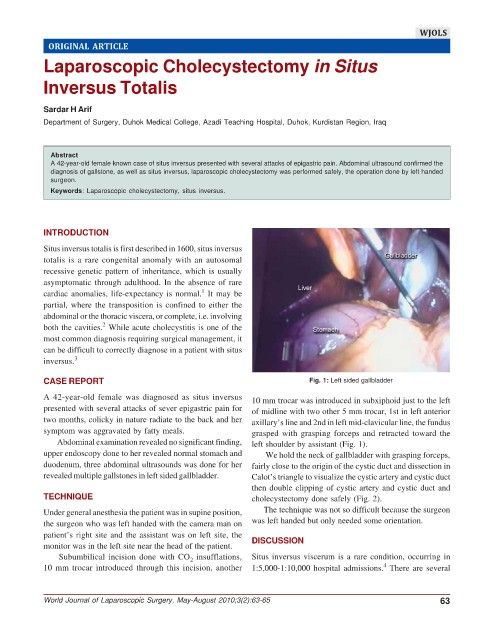
CASE REPORT Fig. 1: Left sided gallbladder
A 42-year-old female was diagnosed as situs inversus 10 mm trocar was introduced in subxiphoid just to the left
presented with several attacks of sever epigastric pain for of midline with two other 5 mm trocar, 1st in left anterior
two months, colicky in nature radiate to the back and her axillary’s line and 2nd in left mid-clavicular line, the fundus
symptom was aggravated by fatty meals. grasped with grasping forceps and retracted toward the
Abdominal examination revealed no significant finding, left shoulder by assistant (Fig. 1).
upper endoscopy done to her revealed normal stomach and We hold the neck of gallbladder with grasping forceps,
duodenum, three abdominal ultrasounds was done for her fairly close to the origin of the cystic duct and dissection in
revealed multiple gallstones in left sided gallbladder. Calot’s triangle to visualize the cystic artery and cystic duct
then double clipping of cystic artery and cystic duct and
TECHNIQUE cholecystectomy done safely (Fig. 2).
Under general anesthesia the patient was in supine position, The technique was not so difficult because the surgeon
the surgeon who was left handed with the camera man on was left handed but only needed some orientation.
patient’s right site and the assistant was on left site, the DISCUSSION
monitor was in the left site near the head of the patient.
Subumbilical incision done with CO insufflations, Situs inversus viscerum is a rare condition, occurring in
2
4
10 mm trocar introduced through this incision, another 1:5,000-1:10,000 hospital admissions. There are several
World Journal of Laparoscopic Surgery, May-August 2010;3(2):63-65 63