
Page 46 - World's Most Popular Laparoscopic Journal
P. 46
Tissue Glue in Laparoscopic Inguinal Hernia Repair: A Retrospective Comparative Analysis
Table 2: Amount of fibrin sealent required vessels) at the level of the transverse umbilical line just lateral
Maximum size of the Required package sizes of to the rectus sheath. The 5 to 12 mm operative trocar is
area to be sealed fibrin sealant always placed on the right hand side for both unilateral and
4 cm 2 0.5 ml bilateral hernias, and a 5 mm trocar is placed on the opposite
8 cm 2 1.0 ml side. For bilateral hernias, the two operative trocars are
16 cm 2 2.0 ml placed about 1 cm below the transverse umbilical line. For
40 cm 2 5.0 ml
a unilateral hernia, the trocar would be positioned 1 cm
above the line, at the intersection with the midclavear line to
Commercially, fibrin sealant is available under the trade create the classic triangulation of base ball diamond concept
name of Tisseel, marketed by Baxter and is supplied in four aimed at the surgical field with the trocars. The assistant
different package sizes of 0.5, 1.0, 2.0 and 5.0 ml, containing operates the scope from the opposite side of the table.
the following components: Evaluation of inguinal regions allows all defects of the
• Tisseel Kit 0.5 for 0.5 ml of reconstituted Tisseel solution transversalis fascia to be detected. The main landmarks are
and 0.5 ml thrombin solution. the remnants of umbilical artery, the ligament of Cooper,
• Tisseel Kit 1.0 for 1.0 ml of reconstituted Tisseel solution epigastric vessels, and the anteriosuperior iliac spine, all of
and 1.0 ml thrombin solution. which also allow definition of the hernia type.
• Tisseel Kit 2.0 for 2.0 ml of reconstituted Tisseel solution
and 2.0 ml thrombin solution. Incision of the Peritoneum
• Tisseel Kit 5.0 for 5.0 ml of reconstituted Tisseel solution If the hernia defect is on the right side, after the iliac spine
and 5.0 ml thrombin solution. is located by external pressure, the peritoneum is incised
OPERATIVE TECHNIQUE TAPP WITH FIBRIN with the scissors at this point, and the incision is continued
GLUE MESH FIXATION horizontally and medially. For a left-sided defect, the incision
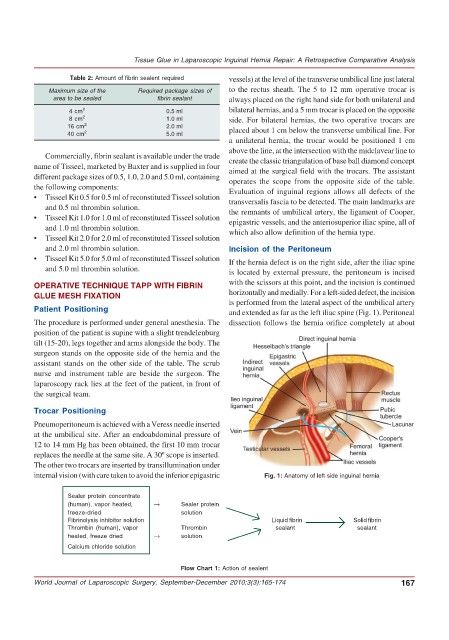
is performed from the lateral aspect of the umbilical artery
Patient Positioning and extended as far as the left iliac spine (Fig. 1). Peritoneal
The procedure is performed under general anesthesia. The dissection follows the hernia orifice completely at about
position of the patient is supine with a slight trendelenburg
tilt (15-20), legs together and arms alongside the body. The
surgeon stands on the opposite side of the hernia and the
assistant stands on the other side of the table. The scrub
nurse and instrument table are beside the surgeon. The
laparoscopy rack lies at the feet of the patient, in front of
the surgical team.
Trocar Positioning
Pneumoperitoneum is achieved with a Veress needle inserted
at the umbilical site. After an endoabdominal pressure of
12 to 14 mm Hg has been obtained, the first 10 mm trocar
replaces the needle at the same site. A 30º scope is inserted.
The other two trocars are inserted by transillumination under
internal vision (with care taken to avoid the inferior epigastric Fig. 1: Anatomy of left side inguinal hernia
Sealer protein concentrate
(human), vapor heated, → Sealer protein
freeze-dried solution
Fibrinolysis inhibitor solution Liquid fibrin Solid fibrin
Thrombin (human), vapor Thrombin sealant sealant
heated, freeze dried → solution
Calcium chloride solution
Flow Chart 1: Action of sealent
World Journal of Laparoscopic Surgery, September-December 2010;3(3):165-174 167