
Page 48 - World's Most Popular Laparoscopic Journal
P. 48
Tissue Glue in Laparoscopic Inguinal Hernia Repair: A Retrospective Comparative Analysis
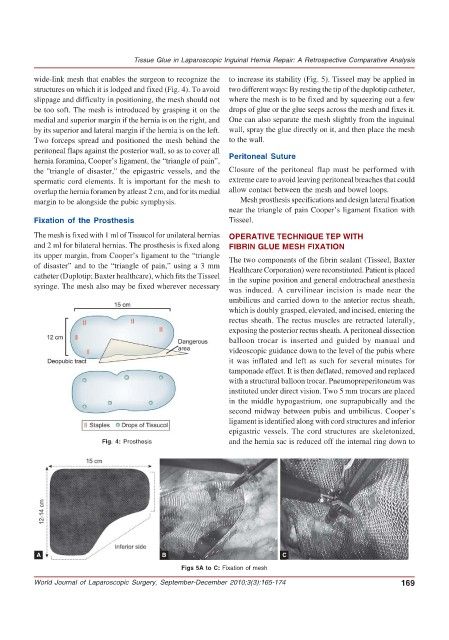
wide-link mesh that enables the surgeon to recognize the to increase its stability (Fig. 5). Tisseel may be applied in
structures on which it is lodged and fixed (Fig. 4). To avoid two different ways: By resting the tip of the duplotip catheter,
slippage and difficulty in positioning, the mesh should not where the mesh is to be fixed and by squeezing out a few
be too soft. The mesh is introduced by grasping it on the drops of glue or the glue seeps across the mesh and fixes it.
medial and superior margin if the hernia is on the right, and One can also separate the mesh slightly from the inguinal
by its superior and lateral margin if the hernia is on the left. wall, spray the glue directly on it, and then place the mesh
Two forceps spread and positioned the mesh behind the to the wall.
peritoneal flaps against the posterior wall, so as to cover all
hernia foramina, Cooper’s ligament, the “triangle of pain”, Peritoneal Suture
the ''triangle of disaster,'' the epigastric vessels, and the Closure of the peritoneal flap must be performed with
spermatic cord elements. It is important for the mesh to extreme care to avoid leaving peritoneal breaches that could
overlap the hernia foramen by atleast 2 cm, and for its medial allow contact between the mesh and bowel loops.
margin to be alongside the pubic symphysis. Mesh prosthesis specifications and design lateral fixation
near the triangle of pain Cooper’s ligament fixation with
Fixation of the Prosthesis Tisseel.
The mesh is fixed with 1 ml of Tissucol for unilateral hernias OPERATIVE TECHNIQUE TEP WITH
and 2 ml for bilateral hernias. The prosthesis is fixed along FIBRIN GLUE MESH FIXATION
its upper margin, from Cooper’s ligament to the “triangle The two components of the fibrin sealant (Tisseel, Baxter
of disaster” and to the “triangle of pain,” using a 3 mm Healthcare Corporation) were reconstituted. Patient is placed
catheter (Duplotip; Baxter healthcare), which fits the Tisseel in the supine position and general endotracheal anesthesia
syringe. The mesh also may be fixed wherever necessary was induced. A curvilinear incision is made near the
umbilicus and carried down to the anterior rectus sheath,
which is doubly grasped, elevated, and incised, entering the
rectus sheath. The rectus muscles are retracted laterally,
exposing the posterior rectus sheath. A peritoneal dissection
balloon trocar is inserted and guided by manual and
videoscopic guidance down to the level of the pubis where
it was inflated and left as such for several minutes for
tamponade effect. It is then deflated, removed and replaced
with a structural balloon trocar. Pneumopreperitoneum was
instituted under direct vision. Two 5 mm trocars are placed
in the middle hypogastrium, one suprapubically and the
second midway between pubis and umbilicus. Cooper’s
ligament is identified along with cord structures and inferior
epigastric vessels. The cord structures are skeletonized,
Fig. 4: Prosthesis and the hernia sac is reduced off the internal ring down to
A B C
Figs 5A to C: Fixation of mesh
World Journal of Laparoscopic Surgery, September-December 2010;3(3):165-174 169