
Page 4 - Journal of WALS
P. 4
Bharati V Hiremath et al
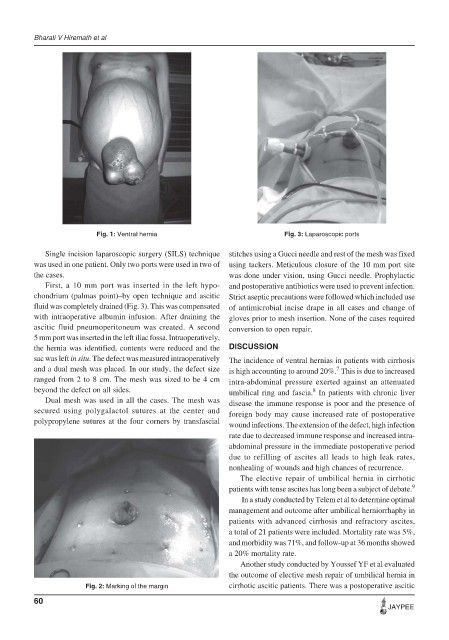
Fig. 1: Ventral hernia Fig. 3: Laparoscopic ports
Single incision laparoscopic surgery (SILS) technique stitches using a Gucci needle and rest of the mesh was fixed
was used in one patient. Only two ports were used in two of using tackers. Meticulous closure of the 10 mm port site
the cases. was done under vision, using Gucci needle. Prophylactic
First, a 10 mm port was inserted in the left hypo- and postoperative antibiotics were used to prevent infection.
chondrium (palmas point)–by open technique and ascitic Strict aseptic precautions were followed which included use
fluid was completely drained (Fig. 3). This was compensated of antimicrobial incise drape in all cases and change of
with intraoperative albumin infusion. After draining the gloves prior to mesh insertion. None of the cases required
ascitic fluid pneumoperitoneum was created. A second conversion to open repair.
5 mm port was inserted in the left iliac fossa. Intraoperatively,
the hernia was identified, contents were reduced and the DISCUSSION
sac was left in situ. The defect was measured intraoperatively The incidence of ventral hernias in patients with cirrhosis
and a dual mesh was placed. In our study, the defect size is high accounting to around 20%. This is due to increased
7
ranged from 2 to 8 cm. The mesh was sized to be 4 cm intra-abdominal pressure exerted against an attenuated
beyond the defect on all sides. umbilical ring and fascia. In patients with chronic liver
8
Dual mesh was used in all the cases. The mesh was disease the immune response is poor and the presence of
secured using polygalactol sutures at the center and foreign body may cause increased rate of postoperative
polypropylene sutures at the four corners by transfascial
wound infections. The extension of the defect, high infection
rate due to decreased immune response and increased intra-
abdominal pressure in the immediate postoperative period
due to refilling of ascites all leads to high leak rates,
nonhealing of wounds and high chances of recurrence.
The elective repair of umbilical hernia in cirrhotic
patients with tense ascites has long been a subject of debate. 9
In a study conducted by Telem et al to determine optimal
management and outcome after umbilical herniorrhaphy in
patients with advanced cirrhosis and refractory ascites,
a total of 21 patients were included. Mortality rate was 5%,
and morbidity was 71%, and follow-up at 36 months showed
a 20% mortality rate.
Another study conducted by Youssef YF et al evaluated
the outcome of elective mesh repair of umbilical hernia in
Fig. 2: Marking of the margin cirrhotic ascitic patients. There was a postoperative ascitic
60
JAYPEE