
Page 7 - WJOLS
P. 7
WJOLS
Gastric Plication as a New Stand-Alone Procedure for the Treatment of Morbid Obesity
2. The last point of the plication (Figs 6C and D) is stopped stomach is better calibrated. The final restricted volume
3 cm before the pylorus. This distance prevents gastric is reached by the end of the first row of separated stitches
obstruction by fold invagination into the pylorus. The before edema and venous stasis installation.
angulus points are ath risk of obstruction to because of Moreover, symmetry of the plicated stomach is better
gastric wall thickness at this level. obtained by making separated stitches. Asymmetry will lead
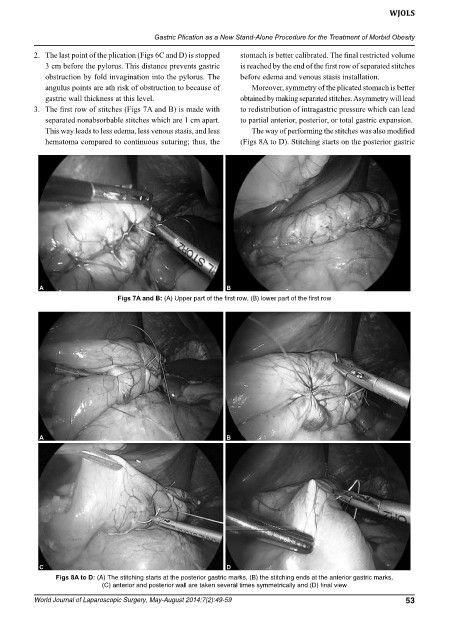
3. The first row of stitches (Figs 7A and B) is made with to redistribution of intragastric pressure which can lead
separated nonabsorbable stitches which are 1 cm apart. to partial anterior, posterior, or total gastric expansion.
This way leads to less edema, less venous stasis, and less The way of performing the stitches was also modified
hematoma compared to continuous suturing; thus, the (Figs 8A to D). Stitching starts on the posterior gastric
A B
Figs 7A and B: (A) Upper part of the first row, (B) lower part of the first row
A B
C D
Figs 8A to D: (A) The stitching starts at the posterior gastric marks, (B) the stitching ends at the anterior gastric marks,
(C) anterior and posterior wall are taken several times symmetrically and (D) final view
World Journal of Laparoscopic Surgery, May-August 2014;7(2):49-59 53