
Page 12 - WJOLS
P. 12
Youssef A Andraos et al
Minor Complications
• Nausea (13.99%)
• Vomiting (12.86%)
• Minor hematemesis (8.53%)
• Hiccup (4.45%)
• Sialorrhea (8.53%)
• Melena (5.25%)
• Diarrhea (3.46%)
• Gastric spasm (3.24%)
DIScuSSION
General overview of the results: In the overall group, a signi-
ficant increase in the percentage of EWL was noted, and
consequently a decrease in body weight, until 12 months
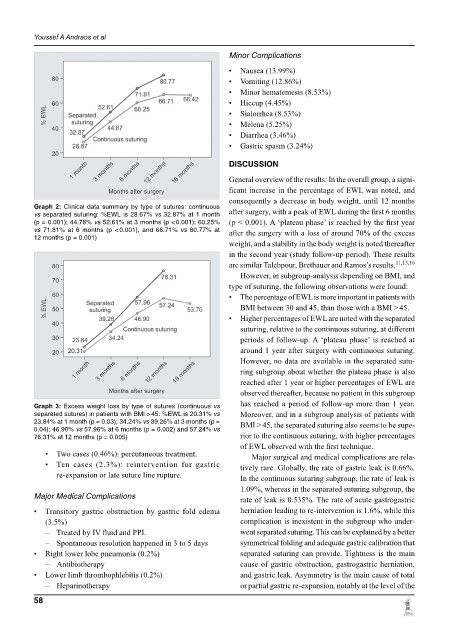
Graph 2: Clinical data summary by type of sutures: continuous
vs separated suturing: %EWL is 28.67% vs 32.87% at 1 month after surgery, with a peak of EWL during the first 6 months
(p = 0.001); 44.78% vs 52.61% at 3 months (p < 0.001); 60.25% (p < 0.001). A ‘plateau phase’ is reached by the first year
vs 71.81% at 6 months (p < 0.001), and 66.71% vs 80.77% at after the surgery with a loss of around 70% of the excess
12 months (p = 0.001)
weight, and a stability in the body weight is noted thereafter
in the second year (study follow-up period). These results
are similar Talebpour, Brethauer and Ramos’s results. 11,13,16
However, in subgroup-analysis depending on BMI, and
type of suturing, the following observations were found:
• The percentage of EWL is more important in patients with
BMI between 30 and 45, than those with a BMI > 45.
• Higher percentages of EWL are noted with the separated
suturing, relative to the continuous suturing, at diffe rent
periods of follow-up. A ‘plateau phase’ is reached at
around 1 year after surgery with continuous suturing.
However, no data are available in the separated sutu-
ring subgroup about whether the plateau phase is also
reached after 1 year or higher percentages of EWL are
observed thereafter, because no patient in this subgroup
has reached a period of follow-up more than 1 year.
Graph 3: Excess weight loss by type of sutures (continuous vs
separated sutures) in patients with BMI > 45: %EWL is 20.31% vs Moreover, and in a subgroup analysis of patients with
23.84% at 1 month (p = 0.03); 34.24% vs 39.26% at 3 months (p = BMI > 45, the separated suturing also seems to be supe-
0.04); 46.90% vs 57.96% at 6 months (p = 0.002) and 57.24% vs
76.31% at 12 months (p = 0.005) rior to the continuous suturing, with higher percentages
of EWL observed with the first technique.
• Two cases (0.46%): percutaneous treatment. Major surgical and medical complications are rela-
• Ten cases (2.3%): reintervention for gastric tively rare. Globally, the rate of gastric leak is 0.66%.
re-expansion or late suture line rupture. In the continuous suturing subgroup, the rate of leak is
1.09%, whereas in the separated suturing subgroup, the
Major Medical Complications rate of leak is 0.535%. The rate of acute gastrogastric
• Transitory gastric obstruction by gastric fold edema herniation leading to re-intervention is 1.6%, while this
(3.5%) complication is inexistent in the subgroup who under-
– Treated by IV fluid and PPI. went separated suturing. This can be explained by a better
– Spontaneous resolution happened in 3 to 5 days symmetrical folding and adequate gastric calibration that
• Right lower lobe pneumonia (0.2%) separated suturing can provide. Tightness is the main
– Antibiotherapy cause of gastric obstruction, gastrogastric herniation,
• Lower limb thrombophlebitis (0.2%) and gastric leak. Asymmetry is the main cause of total
– Heparinotherapy or partial gastric re-expansion, notably at the level of the
58