
Page 4 - WJOLS
P. 4
Youssef A Andraos et al
show that it is effective on excess weight loss (EWL) and
is associated with a low rate of complications. 4,5,19-22
This case series highlights technical steps, results and
complication management of this procedure.
MATeRIAlS AND MeThODS
Study patients and endpoints: The present case-series
study received the approval of the local ethics commit-
tee and was conducted using the National Institute of
Health (NIH) inclusion criteria for bariatric surgery, 15,23,24
the United States Food and Drug Administration (FDA)
appro val of Adjustable Gastric Band (AGB) and the ASMBS
position regarding bariatric surgery in class 1 obesity (BMI
2 24
30-35 kg/m ). Fig. 3: Trocars placement
A total of 482 patients underwent laparoscopic greater
curvature plication (LGCP) from December 13, 2010 to Trocar Placement (Fig. 3)
February 4, 2013. Thirty-three cases were excluded for pre- A five-trocar port technique was used for all patients except
vious bariatric surgery. A total of 449 patients responded to those with a small left liver for whom a three-trocar tech-
inclusion criteria and are included in the study. Results and nique was adopted.
complications were recorded till the end of the second year.
Dissections (Figs 4A to G)
Surgical Techniques
The greater curvature is completely liberated from gastro-
Patient Installation epiploic and splenic attachments from the gastroesophageal
Patients were placed under general anesthesia in an anti- (GE) junction to 3 cm before the pylorus. The posterior gastric
Trendelenburg position at a 30 to 45º French position. wall was held up and the body of the stomach was freed
com pletely from the gastropancreatic attachment. The pos-
terior fundus was completely liberated from the left crus and
the hiatus was inspected to rule out a hiatal hernia. Repara-
tion of the hiatal hernia was performed at the same time
when found in order to decrease the restricted gastric volume.
Calibration and Plication (Figs 5A to D)
A complete visualization of the whole stomach, anteriorly
and posteriorly, is the key of a good gastric calibration.
Gastric plication was created by the invagination of the
greater curvature over a 36 French calibrating tube. Ante-
A rior and posterior marks on the gastric wall were made by
methylene blue or bipolar coagulation. These marks help
in avoiding the narrowing of the plicated stomach or the
widening of the residual gastric space.
Critical Points
1. The first point of the plication (Figs 6A and B) is started
by a cardio plication in case of cardial enlargement
with GE reflux. If there is no preexisting GE reflux, the
plication is started 1 cm from the GE junction to avoid
dysphagia. In case of hiatal hernia with or without GE
reflux, the gastric hernia is treated by left and right crus
B
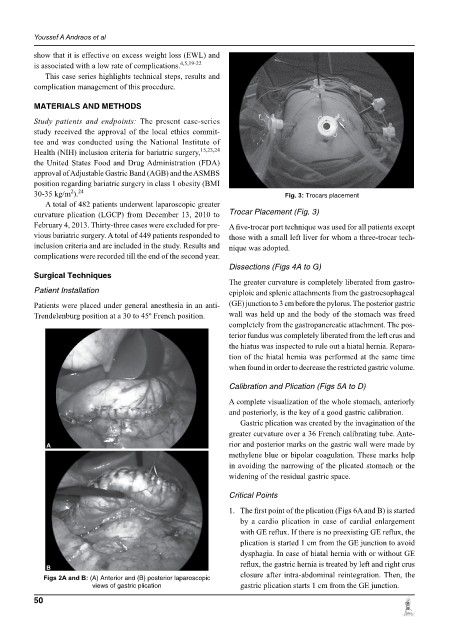
Figs 2A and B: (A) Anterior and (B) posterior laparoscopic closure after intra-abdominal reintegration. Then, the
views of gastric plication gastric plication starts 1 cm from the GE junction.
50