
Page 11 - WJOLS
P. 11
WJOLS
Gastric Plication as a New Stand-Alone Procedure for the Treatment of Morbid Obesity
b. Gastric obstruction (0.4%):
• Due to gastric fold invagination into the lower eso-
phagus (0.2%)
– Treated by laparoscopic deplication and a looser
gastric plication was performed.
• Due to gastric fold invagination into the pylorus (0.2%)
– Treated by deplication.
c. Gastrogastric herniation (0.6%):
• Leading to esogastric leak and peritonitis (0.2%)
– Treated by laparoscopic deplication, gastric suture
and looser plication.
• Leading to gastric hernia necrosis and peritonitis
(0.2%).
– Treated by gastric resection of necrotic herniation,
and deplication.
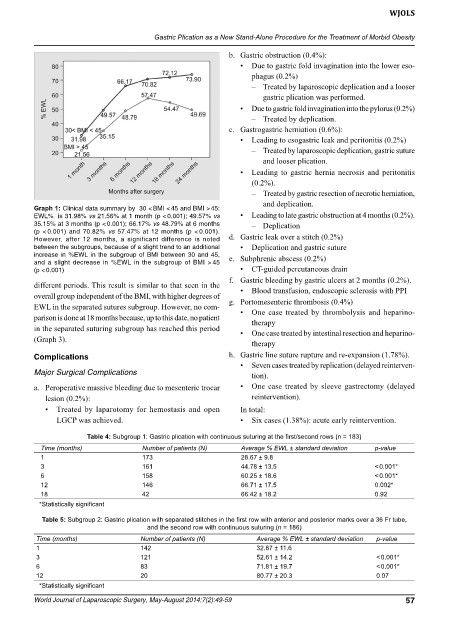
Graph 1: Clinical data summary by 30 < BMI < 45 and BMI > 45:
EWL% is 31.98% vs 21.56% at 1 month (p < 0.001); 49.57% vs • Leading to late gastric obstruction at 4 months (0.2%).
35.15% at 3 months (p < 0.001); 66.17% vs 48.79% at 6 months – Deplication
(p < 0.001) and 70.82% vs 57.47% at 12 months (p < 0.001).
However, after 12 months, a significant difference is noted d. Gastric leak over a stitch (0.2%)
between the subgroups, because of a slight trend to an additional • Deplication and gastric suture
increase in %EWL in the subgroup of BMI between 30 and 45, e. Subphrenic abscess (0.2%)
and a slight decrease in %EWL in the subgroup of BMI > 45
(p < 0.001) • CT-guided percutaneous drain
f. Gastric bleeding by gastric ulcers at 2 months (0.2%).
different periods. This result is similar to that seen in the
• Blood transfusion, endoscopic sclerosis with PPI
overall group independent of the BMI, with higher degrees of g. Portomesenteric thrombosis (0.4%)
EWL in the separated sutures subgroup. However, no com- • One case treated by thrombolysis and heparino-
parison is done at 18 months because, up to this date, no patient therapy
in the separated suturing subgroup has reached this period • One case treated by intestinal resection and heparino-
(Graph 3).
therapy
complications h. Gastric line suture rupture and re-expansion (1.78%).
• Seven cases treated by replication (delayed reinterven-
Major Surgical Complications tion).
a. Peroperative massive bleeding due to mesenteric trocar • One case treated by sleeve gastrectomy (delayed
lesion (0.2%): reintervention).
• Treated by laparotomy for hemostasis and open In total:
LGCP was achieved. • Six cases (1.38%): acute early reintervention.
Table 4: Subgroup 1: Gastric plication with continuous suturing at the first/second rows (n = 183)
Time (months) Number of patients (N) Average % EWL ± standard deviation p-value
1 173 28.67 ± 9.8
3 161 44.78 ± 13.5 < 0.001*
6 158 60.25 ± 18.6 < 0.001*
12 146 66.71 ± 17.5 0.002*
18 42 66.42 ± 18.2 0.92
*Statistically significant
Table 5: Subgroup 2: Gastric plication with separated stitches in the first row with anterior and posterior marks over a 36 Fr tube,
and the second row with continuous suturing (n = 186)
Time (months) Number of patients (N) Average % EWL ± standard deviation p-value
1 142 32.87 ± 11.6
3 121 52.61 ± 14.2 < 0.001*
6 83 71.81 ± 19.7 < 0.001*
12 20 80.77 ± 20.3 0.07
*Statistically significant
World Journal of Laparoscopic Surgery, May-August 2014;7(2):49-59 57