
Page 16 - WJOLS
P. 16
Ahmad Jameel Ismail, RK Mishra
registered animal breeding houses and conduct of the axillary line and the target port at the 3rd intercostal space
research was obtained. At the end of the experiments eutha- along the midclavicular line (Fig. 3).
nasia was induced and the animal carcasses were disposed
according to the provisions. Port Placement in VATS Heller’s Esophagocar-
The animals were anesthetized (ketamine, propofol, diomyotomy
diazepam, midazolam and tramadol). The ports were created The ports placement for VATS Heller’s esophagocardio-
using surgical scalpel and air was insufflated into the chest myotomy by the BDP requires putting the optical port at 7th
cavity to collapse the ipsilateral lung. The optical trocar intercostal space along the midaxillary line, the 1st working
was inserted blindly while the working ports were inserted port at the 8th intercostal space along the posterior axillary
under vision. Pericardial window was done using a grasper line and the 2nd working port at the 6th intercostal space
and a scissors. esophagocardiomyotomy was done with along the posterior axillary line.
the alternating use of scissors, monopolar hook diathermy The TTP requires placing the optical port at the 7th inter-
and grasper for retracting the lower lobe of the left lung. costal space along the midaxillary line, the 1st working
Monopolar hook diathermy was used to do thoracic sym- port at the 8th intercostal space along the posterior axillary
pathectomy. At the end of the procedure euthanasia was line and the target port at the 5th intercostal space along the
conducted by giving high dose of succinylcholine and the midaxillary line (Fig. 4).
carcasses disposed appropriately.
There are some limitations of this research which include: Port Placement in VATS
(i) the small sample size because the study is on animal Thoracic Sympathectomy
models which are not commonly used now because of strin-
gent legislations and the limited time (ii) swine models have The ports placement for VATS thoracic sympathectomy by
flimsy tissues and are easily injured and the space between the BDP requires putting the optical port at 5th intercostal
the anterior and posterior axillary lines are shorter which space along the midaxillary line, the 1st working port at the
limit exposure. 4th intercostal space along the posterior axillary line and
the 2nd working port at the 3rd intercostal space along the
BDP vs TTP anterior axillary line.
Port Placement in VATS Pericardial Window The TTP requires placing the optical port at the 7th inter-
costal space along the anterior axillary line, the 1st working
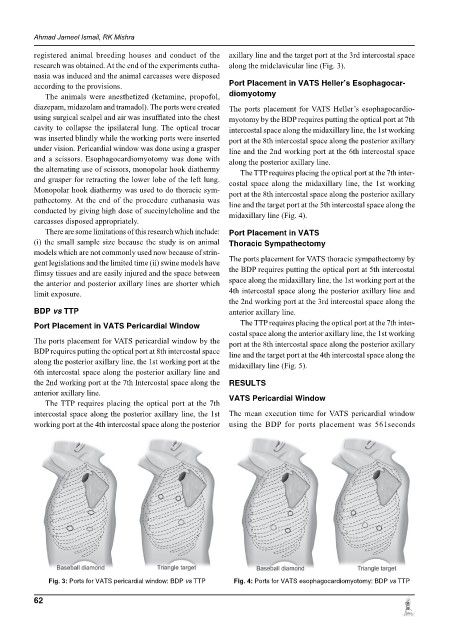
The ports placement for VATS pericardial window by the port at the 8th intercostal space along the posterior axillary
BDP requires putting the optical port at 8th intercostal space line and the target port at the 4th intercostal space along the
along the posterior axillary line, the 1st working port at the midaxillary line (Fig. 5).
6th intercostal space along the posterior axillary line and
the 2nd working port at the 7th Intercostal space along the RESULTS
anterior axillary line. VATS Pericardial Window
The TTP requires placing the optical port at the 7th
intercostal space along the posterior axillary line, the 1st The mean execution time for VATS pericardial window
working port at the 4th intercostal space along the posterior using the BDP for ports placement was 561seconds
Fig. 3: Ports for VATS pericardial window: BDP vs TTP Fig. 4: Ports for VATS esophagocardiomyotomy: BDP vs TTP
62