
Page 32 - Laparoscopic Journal - WJOLS
P. 32
Njem Josiah Miner, RK Mishra
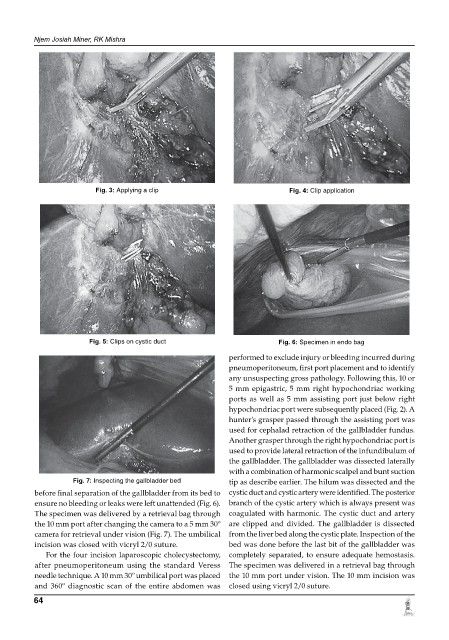
Fig. 3: applying a clip Fig. 4: clip application
Fig. 5: clips on cystic duct Fig. 6: specimen in endo bag
performed to exclude injury or bleeding incurred during
pneumoperitoneum, first port placement and to identify
any unsuspecting gross pathology. Following this, 10 or
5 mm epigastric, 5 mm right hypochondriac working
ports as well as 5 mm assisting port just below right
hypochondriac port were subsequently placed (Fig. 2). A
hunter’s grasper passed through the assisting port was
used for cephalad retraction of the gallbladder fundus.
Another grasper through the right hypochondriac port is
used to provide lateral retraction of the infundibulum of
the gallbladder. The gallbladder was dissected laterally
with a combination of harmonic scalpel and bunt suction
Fig. 7: inspecting the gallbladder bed tip as describe earlier. The hilum was dissected and the
before final separation of the gallbladder from its bed to cystic duct and cystic artery were identified. The posterior
ensure no bleeding or leaks were left unattended (Fig. 6). branch of the cystic artery which is always present was
The specimen was delivered by a retrieval bag through coagulated with harmonic. The cystic duct and artery
the 10 mm port after changing the camera to a 5 mm 30º are clipped and divided. The gallbladder is dissected
camera for retrieval under vision (Fig. 7). The umbilical from the liver bed along the cystic plate. Inspection of the
incision was closed with vicryl 2/0 suture. bed was done before the last bit of the gallbladder was
For the four incision laparoscopic cholecystectomy, completely separated, to ensure adequate hemostasis.
after pneumoperitoneum using the standard Veress The specimen was delivered in a retrieval bag through
needle technique. A 10 mm 30º umbilical port was placed the 10 mm port under vision. The 10 mm incision was
and 360º diagnostic scan of the entire abdomen was closed using vicryl 2/0 suture.
64