
Page 38 - WJOLS - Laparoscopic Journal
P. 38
Mandavi Rai
Direct Trocar Entry Technique write to the manufacturers of shielded laparoscopic
trocars requested that in the absence of clinical data
This technique was introduced by Dingerfield in 1978. In
his first publication, he suggested the advantages of his showing reduced incidence of injuries, manufacturers
technique which eliminates Veress needle complications, and distributors voluntary eliminate safety claims from
19
the label of shielded trocars (Fig. 3).
these include failed pneumoperitoneum, preperitoneal
insufflation and gas embolism. It is fast as it is a one-step
pneumoperitoneum. However, being a blind procedure Visual Entry Systems (Visiport)
it does not eliminate the risk of bowel and vascular These include the disposable optic trocars and the
injuries. 15,16 Several studies were published stressing endo TIP visual cannula. These new technology aims
on safety of this method and recommending its use for to optimize the laparoscopic entry by facilitating entry
primary access. Most of these studies were retrospective, under direct vision. Controlled randomized trials are
only few studies were prospective. A retrospective required to assess their safety and proof their superiority
review of 51 publications comparing the entryrelated to the traditional Veress needle and trocar/cannula
complications with the closed (Veress/trocar technique, system in order to justify their expensive cost (Fig. 4). 20
open and direct trocar technique). Entryrelated bowel
injury rate were 0.04% (Veress/trocar), 0.11% (open), and Transversus Abdominis Plane Block
0.05% (direct). The corresponding vascular injury rates Abdominal field blocks have been around for a long
17
were 0.04, 0.01 and 0% respectively. From the above time and have been extensively used as they are mostly
studies, there is no clear evidence as to the optimal form technically unchallenging. They, however, provide
of laparoscopy entry in low risk patient and it depends limited analgesic fields, hence multiple injections are
on the surgeon preference and experience with the usually required. Traditionally, these blocks have blind
individual technique. 17
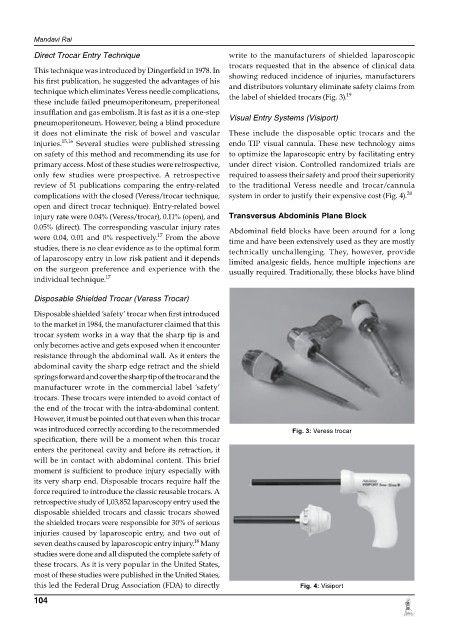
Disposable Shielded Trocar (Veress Trocar)
Disposable shielded ‘safety’ trocar when first introduced
to the market in 1984, the manufacturer claimed that this
trocar system works in a way that the sharp tip is and
only becomes active and gets exposed when it encounter
resistance through the abdominal wall. As it enters the
abdominal cavity the sharp edge retract and the shield
springs forward and cover the sharp tip of the trocar and the
manufacturer wrote in the commercial label ‘safety’
trocars. These trocars were intended to avoid contact of
the end of the trocar with the intraabdominal content.
However, it must be pointed out that even when this trocar
was introduced correctly according to the recommended Fig. 3: Veress trocar
specification, there will be a moment when this trocar
enters the peritoneal cavity and before its retraction, it
will be in contact with abdominal content. This brief
moment is sufficient to produce injury especially with
its very sharp end. Disposable trocars require half the
force required to introduce the classic reusable trocars. A
retrospective study of 1,03,852 laparoscopy entry used the
disposable shielded trocars and classic trocars showed
the shielded trocars were responsible for 30% of serious
injuries caused by laparoscopic entry, and two out of
18
seven deaths caused by laparoscopic entry injury. Many
studies were done and all disputed the complete safety of
these trocars. As it is very popular in the United States,
most of these studies were published in the United States,
this led the Federal Drug Association (FDA) to directly Fig. 4: Visiport
104