
Page 24 - World Journal of Laparoscopic Surgery
P. 24
John Suresh Kumar TR
and with right hand posterior and anterior windows are LC. A three-port LC can be performed by using a suture
created by dissecting in Calot’s triangle. Critical view of for fundal traction, so that the vision of the Calot’s triangle
safety is of utmost important to prevent bile duct injury. is not compromised. The traction suture is inserted from
Clipping of the cystic duct and cystic artery is achieved the right lower chest wall taking care it does not penetrate
from 10 mm epigastric port. Gallbladder extraction is the pleura or the lung in the right anterior or mid-axillary
generally done from either epigastric or umbilical port. line with a straight needle inserted percutaneously or by a
free thread inserted into the abdomen and withdrawn by
Reduced Port Size Laparoscopic a prolene loop inserted through a standard 18 G needle,
Cholecystectomy an epidural needle, or the verees needle. We can also use
1
figure of eight suture on fundus to apply gentle traction.
The size of epigastric trocar is reduced from 10 to 5 mm
and this is claimed to reduce the pain and improve the This avoids the complication of occasional minor bile leak
cosmesis. This requires bipolar coagulation of the cystic while using a traction suture. One can also make use of
artery and 5 mm clip applicator for clipping the cystic stryker mini alligator to provide traction on fundus of
duct or ligation of cystic duct with an extra corporeal the gallbladder.
knot. At the end of the procedure the gallbladder is STRYKER MINI ALLIGATOR
extracted through the umbilical port. Another variant
of this technique is where a 5 mm telescope is used at Some studies show no major advantage in reducing one
the umbilicus and a 10 mm epigastric trocar is used for 5 mm right lumbar port as it neither reduces pain nor
standard clip ligature of the cystic duct and epigastric alters the postoperative recovery and it is cosmetically
extraction of the gallbladder. 1 not superior to the traditional standard four-port LC.
Some other studies have showed advantage of three
2
3,4
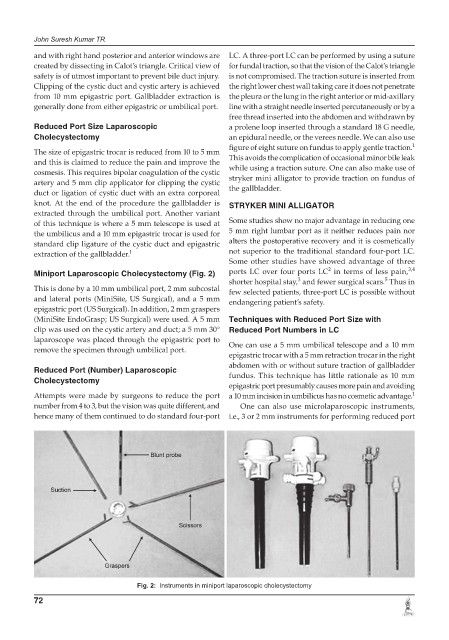
Miniport Laparoscopic Cholecystectomy (Fig. 2) ports LC over four ports LC in terms of less pain,
3
5
shorter hospital stay, and fewer surgical scars. Thus in
This is done by a 10 mm umbilical port, 2 mm subcostal few selected patients, three-port LC is possible without
and lateral ports (MiniSite, US Surgical), and a 5 mm endangering patient’s safety.
epigastric port (US Surgical). In addition, 2 mm graspers
(MiniSite EndoGrasp; US Surgical) were used. A 5 mm Techniques with Reduced Port Size with
clip was used on the cystic artery and duct; a 5 mm 30° Reduced Port Numbers in LC
laparoscope was placed through the epigastric port to One can use a 5 mm umbilical telescope and a 10 mm
remove the specimen through umbilical port.
epigastric trocar with a 5 mm retraction trocar in the right
abdomen with or without suture traction of gallbladder
Reduced Port (Number) Laparoscopic fundus. This technique has little rationale as 10 mm
Cholecystectomy
epigastric port presumably causes more pain and avoiding
Attempts were made by surgeons to reduce the port a 10 mm incision in umbilicus has no cosmetic advantage. 1
number from 4 to 3, but the vision was quite different, and One can also use microlaparoscopic instruments,
hence many of them continued to do standard four-port i.e., 3 or 2 mm instruments for performing reduced port
Fig. 2: Instruments in miniport laparoscopic cholecystectomy
72