
Page 43 - Journal of Laparoscopic Surgery
P. 43
WJOLS
Laparoscopic Port Closure Techniques and Incidence of Port-site Hernias: A Review and Recommendations
The suture end is held in the loop of the thread which grasped and pulled through the incision and facilitates
is in the Veress and is pulled out through the skin incision the passage of the needle.
and tied externally under vision. They report no incidence
of port-site hernia or any other complications. Suture Carrier
27
Jorge et al. and Li and Chung developed this carrier
Maciol Suture Needle Set
which made use of the vertical space. This is a hook
24
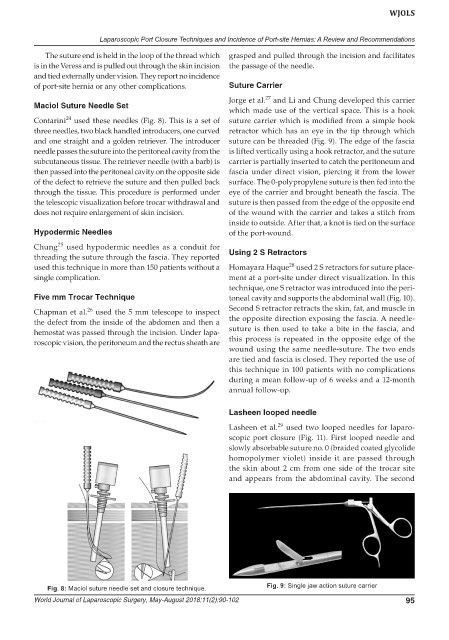
Contarini used these needles (Fig. 8). This is a set of suture carrier which is modified from a simple hook
three needles, two black handled introducers, one curved retractor which has an eye in the tip through which
and one straight and a golden retriever. The introducer suture can be threaded (Fig. 9). The edge of the fascia
needle passes the suture into the peritoneal cavity from the is lifted vertically using a hook retractor, and the suture
subcutaneous tissue. The retriever needle (with a barb) is carrier is partially inserted to catch the peritoneum and
then passed into the peritoneal cavity on the opposite side fascia under direct vision, piercing it from the lower
of the defect to retrieve the suture and then pulled back surface. The 0-polypropylene suture is then fed into the
through the tissue. This procedure is performed under eye of the carrier and brought beneath the fascia. The
the telescopic visualization before trocar withdrawal and suture is then passed from the edge of the opposite end
does not require enlargement of skin incision. of the wound with the carrier and takes a stitch from
inside to outside. After that, a knot is tied on the surface
Hypodermic Needles of the port-wound.
25
Chung used hypodermic needles as a conduit for
threading the suture through the fascia. They reported Using 2 S Retractors
28
used this technique in more than 150 patients without a Homayara Haque used 2 S retractors for suture place-
single complication. ment at a port-site under direct visualization. In this
technique, one S retractor was introduced into the peri-
Five mm Trocar Technique toneal cavity and supports the abdominal wall (Fig. 10).
26
Chapman et al. used the 5 mm telescope to inspect Second S retractor retracts the skin, fat, and muscle in
the defect from the inside of the abdomen and then a the opposite direction exposing the fascia. A needle-
hemostat was passed through the incision. Under lapa- suture is then used to take a bite in the fascia, and
roscopic vision, the peritoneum and the rectus sheath are this process is repeated in the opposite edge of the
wound using the same needle-suture. The two ends
are tied and fascia is closed. They reported the use of
this technique in 100 patients with no complications
during a mean follow-up of 6 weeks and a 12-month
annual follow-up.
Lasheen looped needle
29
Lasheen et al. used two looped needles for laparo-
scopic port closure (Fig. 11). First looped needle and
slowly absorbable suture no. 0 (braided coated glycolide
homopolymer violet) inside it are passed through
the skin about 2 cm from one side of the trocar site
and appears from the abdominal cavity. The second
Fig. 8: Maciol suture needle set and closure technique. Fig. 9: Single jaw action suture carrier
World Journal of Laparoscopic Surgery, May-August 2018;11(2):90-102 95