
Page 42 - Journal of Laparoscopic Surgery
P. 42
Mohammed Arifuzaman, Asna Samreen
Pneumoperitoneum is maintained. The closed peri- in the port-site and deployed with the wings which lock
toneal layer is viewed through the laparoscope, and in the abdominal wall. The sutures are fully inserted
palpation of the closure ensures that the fascial layer into the guide channels and locked. The retriever is then
is completely occluded. The author reports the use of removed and the same process continued on the other
this technique in more than 200 advanced laparoscopic side. The wing shield is the collapsed once the slide lock
techniques without a single case of port-site hernia. is repositioned and the device removed from the defect.
And also been introduced, that is Carter–Thomason II, Both the ends of the suture are then tied, and the knot
which offers better and faster closure (Fig. 6). It has a buries deep in the fascial layer. This study was performed
15 mm and 10 mm suture guides and a suture passer. The in cadavers and reportedly better results were obtained
suture passer useful in obese patients. with EFx than CT in terms of time needed for closure,
safety, and facility.
Endo Close Instrument 22
Del Junco M published a study, where the efficacy of Veress Needle for Port-site Closure 23
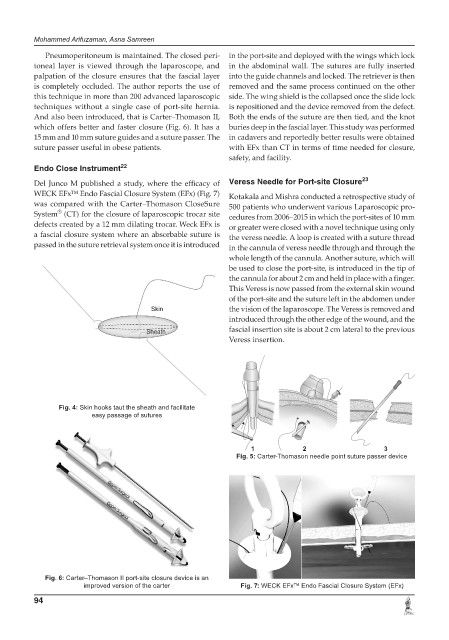
WECK EFx™ Endo Fascial Closure System (EFx) (Fig. 7) Kotakala and Mishra conducted a retrospective study of
was compared with the Carter–Thomason CloseSure 500 patients who underwent various Laparoscopic pro-
®
System (CT) for the closure of laparoscopic trocar site cedures from 2006–2015 in which the port-sites of 10 mm
defects created by a 12 mm dilating trocar. Weck EFx is or greater were closed with a novel technique using only
a fascial closure system where an absorbable suture is the veress needle. A loop is created with a suture thread
passed in the suture retrieval system once it is introduced in the cannula of veress needle through and through the
whole length of the cannula. Another suture, which will
be used to close the port-site, is introduced in the tip of
the cannula for about 2 cm and held in place with a finger.
This Veress is now passed from the external skin wound
of the port-site and the suture left in the abdomen under
the vision of the laparoscope. The Veress is removed and
introduced through the other edge of the wound, and the
fascial insertion site is about 2 cm lateral to the previous
Veress insertion.
Fig. 4: Skin hooks taut the sheath and facilitate
easy passage of sutures
1 2 3
Fig. 5: Carter-Thomason needle point suture passer device
Fig. 6: Carter–Thomason II port-site closure device is an
improved version of the carter Fig. 7: WECK EFx™ Endo Fascial Closure System (EFx)
94