
Page 18 - WJOLS - World Journal of Laparoscopic Surgery
P. 18
Laparoscopic Inguinal Hernia
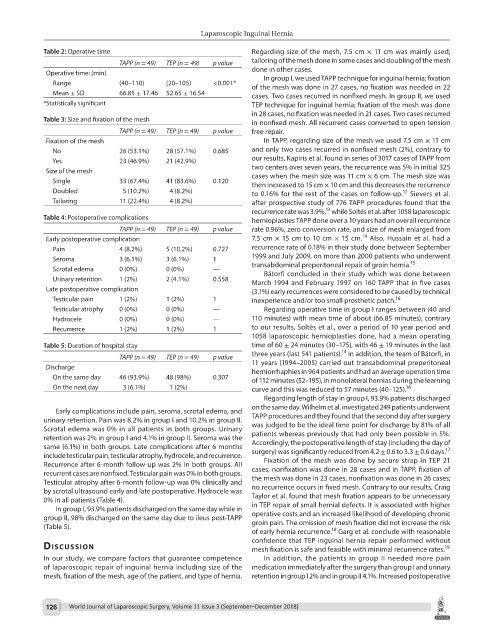
Table 2: Operative time Regarding size of the mesh, 7.5 cm × 11 cm was mainly used;
TAPP (n = 49) TEP (n = 49) p value tailoring of the mesh done in some cases and doubling of the mesh
Operative time: (min) done in other cases.
In group I, we used TAPP technique for inguinal hernia; fixation
Range (40–110) (20–105) <0.001* of the mesh was done in 27 cases, no fixation was needed in 22
Mean ± SD 66.85 ± 17.46 52.65 ± 16.54 cases. Two cases recurred in nonfixed mesh. In group II, we used
*Statistically significant TEP technique for inguinal hernia; fixation of the mesh was done
in 28 cases, no fixation was needed in 21 cases. Two cases recurred
Table 3: Size and fixation of the mesh in nonfixed mesh. All recurrent cases converted to open tension
TAPP (n = 49) TEP (n = 49) p value free repair.
Fixation of the mesh In TAPP, regarding size of the mesh we used 7.5 cm × 11 cm
No 26 (53.1%) 28 (57.1%) 0.685 and only two cases recurred in nonfixed mesh (2%), contrary to
Yes 23 (46.9%) 21 (42.9%) our results, Kapiris et al. found in series of 3017 cases of TAPP from
Size of the mesh two centers over seven years, the recurrence was 5% in initial 325
cases when the mesh size was 11 cm × 6 cm. The mesh size was
Single 33 (67.4%) 41 (83.6%) 0.120 then increased to 15 cm × 10 cm and this decreases the recurrence
Doubled 5 (10.2%) 4 (8.2%) to 0.16% for the rest of the cases on follow-up. Sievers et al.
12
Tailoring 11 (22.4%) 4 (8.2%) after prospective study of 776 TAPP procedures found that the
13
recurrence rate was 3.9%, while Soltés et al. after 1058 laparoscopic
Table 4: Postoperative complications hernioplasties TAPP done over a 10 years had an overall recurrence
TAPP (n = 49) TEP (n = 49) p value rate 0.96%, zero conversion rate, and size of mesh enlarged from
14
Early postoperative complication 7.5 cm × 15 cm to 10 cm × 15 cm. Also, Hussain et al. had a
Pain 4 (8.2%) 5 (10.2%) 0.727 recurrence rate of 0.18% in their study done between September
Seroma 3 (6.1%) 3 (6.1%) 1 1999 and July 2009, on more than 2000 patients who underwent
15
Scrotal edema 0 (0%) 0 (0%) — transabdominal preperitoneal repair of groin hernia.
Bátorfi concluded in their study which was done between
Urinary retention 1 (2%) 2 (4.1%) 0.558 March 1994 and February 1997 on 160 TAPP that in five cases
Late postoperative complication (3.1%) early recurrences were considered to be caused by technical
Testicular pain 1 (2%) 1 (2%) 1 inexperience and/or too small prosthetic patch.
16
Testicular atrophy 0 (0%) 0 (0%) — Regarding operative time in group I ranges between (40 and
Hydrocele 0 (0%) 0 (0%) — 110 minutes) with mean time of about (66.85 minutes), contrary
Recurrence 1 (2%) 1 (2%) 1 to our results, Soltés et al., over a period of 10 year period and
1058 laparoscopic hernioplasties done, had a mean operating
Table 5: Duration of hospital stay time of 60 ± 24 minutes (30–175), with 46 ± 19 minutes in the last
14
three years (last 541 patients). In addition, the team of Bátorfi, in
TAPP (n = 49) TEP (n = 49) p value
Discharge 11 years (1994–2005) carried out transabdominal preperitoneal
herniorrhaphies in 964 patients and had an average operation time
On the same day 46 (93.9%) 48 (98%) 0.307 of 112 minutes (52–195), in monolateral hernias during the learning
On the next day 3 (6.1%) 1 (2%) curve and this was reduced to 57 minutes (40–125).
16
Regarding length of stay in group I, 93.9% patients discharged
on the same day. Wilhelm et al. investigated 249 patients underwent
Early complications include pain, seroma, scrotal edema, and
urinary retention. Pain was 8.2% in group I and 10.2% in group II. TAPP procedures and they found that the second day after surgery
Scrotal edema was 0% in all patients in both groups. Urinary was judged to be the ideal time point for discharge by 81% of all
retention was 2% in group I and 4.1% in group II. Seroma was the patients whereas previously that had only been possible in 5%.
same (6.1%) in both groups. Late complications after 6 months Accordingly, the postoperative length of stay (including the day of
17
include testicular pain, testicular atrophy, hydrocele, and recurrence. surgery) was significantly reduced from 4.2 ± 0.6 to 3.3 ± 0.6 days.
Recurrence after 6-month follow-up was 2% in both groups. All Fixation of the mesh was done by secure strap in TEP 21
recurrent cases are nonfixed. Testicular pain was 0% in both groups. cases, nonfixation was done in 28 cases and in TAPP, fixation of
Testicular atrophy after 6-month follow-up was 0% clinically and the mesh was done in 23 cases, nonfixation was done in 26 cases;
by scrotal ultrasound early and late postoperative. Hydrocele was no recurrence occurs in fixed mesh. Contrary to our results, Craig
0% in all patients (Table 4). Taylor et al. found that mesh fixation appears to be unnecessary
In group I, 93.9% patients discharged on the same day while in in TEP repair of small hernial defects. It is associated with higher
group II, 98% discharged on the same day due to ileus post-TAPP operative costs and an increased likelihood of developing chronic
(Table 5). groin pain. The omission of mesh fixation did not increase the risk
18
of early hernia recurrence. Garg et al. conclude with reasonable
confidence that TEP inguinal hernia repair performed without
dIscussIon mesh fixation is safe and feasible with minimal recurrence rates.
19
In our study, we compare factors that guarantee competence In addition, the patients in group II needed more pain
of laparoscopic repair of inguinal hernia including size of the medication immediately after the surgery than group I and urinary
mesh, fixation of the mesh, age of the patient, and type of hernia. retention in group I 2% and in group II 4.1%. Increased postoperative
126 World Journal of Laparoscopic Surgery, Volume 11 Issue 3 (September–December 2018)