
Page 64 - World Journal of Laparoscopic Surgery
P. 64
Laparoscopic Cholecystectomy: How We Do It
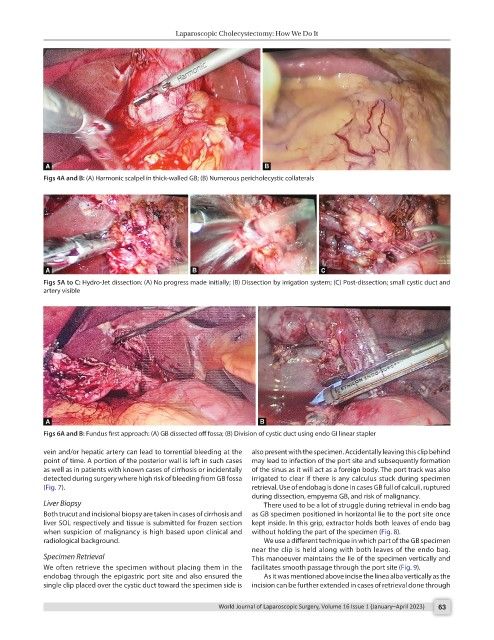
Figs 4A and B: (A) Harmonic scalpel in thick-walled GB; (B) Numerous pericholecystic collaterals
Figs 5A to C: Hydro-Jet dissection: (A) No progress made initially; (B) Dissection by irrigation system; (C) Post-dissection; small cystic duct and
artery visible
Figs 6A and B: Fundus first approach: (A) GB dissected off fossa; (B) Division of cystic duct using endo GI linear stapler
vein and/or hepatic artery can lead to torrential bleeding at the also present with the specimen. Accidentally leaving this clip behind
point of time. A portion of the posterior wall is left in such cases may lead to infection of the port site and subsequently formation
as well as in patients with known cases of cirrhosis or incidentally of the sinus as it will act as a foreign body. The port track was also
detected during surgery where high risk of bleeding from GB fossa irrigated to clear if there is any calculus stuck during specimen
(Fig. 7). retrieval. Use of endobag is done in cases GB full of calculi, ruptured
during dissection, empyema GB, and risk of malignancy.
Liver Biopsy There used to be a lot of struggle during retrieval in endo bag
Both trucut and incisional biopsy are taken in cases of cirrhosis and as GB specimen positioned in horizontal lie to the port site once
liver SOL respectively and tissue is submitted for frozen section kept inside. In this grip, extractor holds both leaves of endo bag
when suspicion of malignancy is high based upon clinical and without holding the part of the specimen (Fig. 8).
radiological background. We use a different technique in which part of the GB specimen
near the clip is held along with both leaves of the endo bag.
Specimen Retrieval This manoeuver maintains the lie of the specimen vertically and
We often retrieve the specimen without placing them in the facilitates smooth passage through the port site (Fig. 9).
endobag through the epigastric port site and also ensured the As it was mentioned above incise the linea alba vertically as the
single clip placed over the cystic duct toward the specimen side is incision can be further extended in cases of retrieval done through
World Journal of Laparoscopic Surgery, Volume 16 Issue 1 (January–April 2023) 63