
Page 65 - World Journal of Laparoscopic Surgery
P. 65
Laparoscopic Cholecystectomy: How We Do It
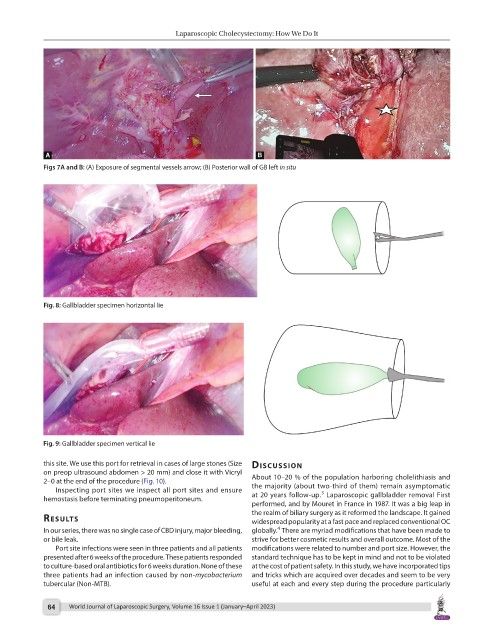
Figs 7A and B: (A) Exposure of segmental vessels arrow; (B) Posterior wall of GB left in situ
Fig. 8: Gallbladder specimen horizontal lie
Fig. 9: Gallbladder specimen vertical lie
this site. We use this port for retrieval in cases of large stones (Size discussion
on preop ultrasound abdomen > 20 mm) and close it with Vicryl
2–0 at the end of the procedure (Fig. 10). About 10–20 % of the population harboring cholelithiasis and
Inspecting port sites we inspect all port sites and ensure the majority (about two-third of them) remain asymptomatic
3
hemostasis before terminating pneumoperitoneum. at 20 years follow-up. Laparoscopic gallbladder removal First
performed, and by Mouret in France in 1987. It was a big leap in
results the realm of biliary surgery as it reformed the landscape. It gained
widespread popularity at a fast pace and replaced conventional OC
4
In our series, there was no single case of CBD injury, major bleeding, globally. There are myriad modifications that have been made to
or bile leak. strive for better cosmetic results and overall outcome. Most of the
Port site infections were seen in three patients and all patients modifications were related to number and port size. However, the
presented after 6 weeks of the procedure. These patients responded standard technique has to be kept in mind and not to be violated
to culture-based oral antibiotics for 6 weeks duration. None of these at the cost of patient safety. In this study, we have incorporated tips
three patients had an infection caused by non-mycobacterium and tricks which are acquired over decades and seem to be very
tubercular (Non-MTB). useful at each and every step during the procedure particularly
64 World Journal of Laparoscopic Surgery, Volume 16 Issue 1 (January–April 2023)