
Page 56 - World Journal of Laparoscopic Surgery
P. 56
Post-TAPP Mesh Hernioplasty Seroma Formation and Its Management
displaces the mesh. As a result, the hernia may recur. Studies have
shown that occurrence of seroma after TAPP is 7.7–17%. Susmalian
7
et al. believed in using ultrasonography for the detection of seroma.
However, they are mostly asymptomatic and are not clinically
meaningful.
Applying pressure bandage, the application of fibrin sealant in
the preperitoneal space, and placing a negative-suction or vacuum
suction drain in the plain of dissection are a few of the procedures
8
described in the literature to prevent seroma formation. But the
drain can only be placed for a short period or else it will lead to
iatrogenic infections. In the inguinoscrotal region, putting on a
compression dressing is not an easy job. Some studies have also
favored the complete dissection of the sac to prevent seroma
formation. But with concomitantly running cord structures, most
importantly the vas deference and the vessels, complete dissection
can lead to unwanted complications like bleeding or transection
of cord structures.
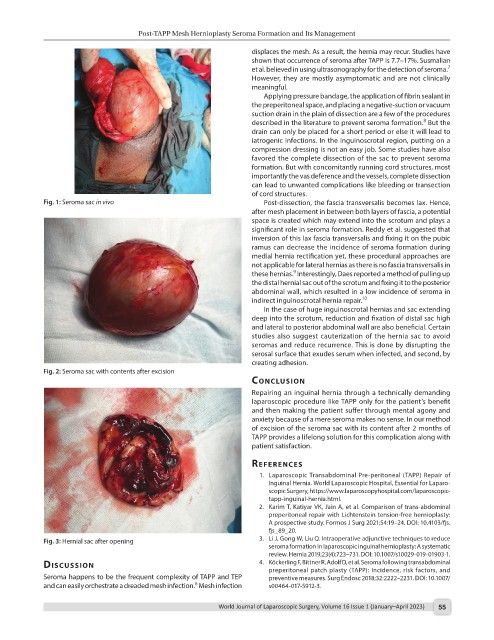
Fig. 1: Seroma sac in vivo Post-dissection, the fascia transversalis becomes lax. Hence,
after mesh placement in between both layers of fascia, a potential
space is created which may extend into the scrotum and plays a
significant role in seroma formation. Reddy et al. suggested that
inversion of this lax fascia transversalis and fixing it on the pubic
ramus can decrease the incidence of seroma formation during
medial hernia rectification yet, these procedural approaches are
not applicable for lateral hernias as there is no fascia transversalis in
9
these hernias. Interestingly, Daes reported a method of pulling up
the distal hernial sac out of the scrotum and fixing it to the posterior
abdominal wall, which resulted in a low incidence of seroma in
indirect inguinoscrotal hernia repair. 10
In the case of huge inguinoscrotal hernias and sac extending
deep into the scrotum, reduction and fixation of distal sac high
and lateral to posterior abdominal wall are also beneficial. Certain
studies also suggest cauterization of the hernia sac to avoid
seromas and reduce recurrence. This is done by disrupting the
serosal surface that exudes serum when infected, and second, by
creating adhesion.
Fig. 2: Seroma sac with contents after excision
conclusIon
Repairing an inguinal hernia through a technically demanding
laparoscopic procedure like TAPP only for the patient’s benefit
and then making the patient suffer through mental agony and
anxiety because of a mere seroma makes no sense. In our method
of excision of the seroma sac with its content after 2 months of
TAPP provides a lifelong solution for this complication along with
patient satisfaction.
references
1. Laparoscopic Transabdominal Pre-peritoneal (TAPP) Repair of
Inguinal Hernia. World Laparoscopic Hospital, Essential for Laparo-
scopic Surgery, https://www.laparoscopyhospital.com/laparoscopic-
tapp-inguinal-hernia.html.
2. Karim T, Katiyar VK, Jain A, et al. Comparison of trans-abdominal
preperitoneal repair with Lichtenstein tension-free hernioplasty:
A prospective study. Formos J Surg 2021;54:19–24. DOI: 10.4103/fjs.
fjs_89_20.
Fig. 3: Hernial sac after opening 3. Li J, Gong W, Liu Q. Intraoperative adjunctive techniques to reduce
seroma formation in laparoscopic inguinal hernioplasty: A systematic
review. Hernia 2019;23(4):723–731. DOI: 10.1007/s10029-019-01903-1.
dIscussIon 4. Köckerling F, Bittner R, Adolf D, et al. Seroma following transabdominal
preperitoneal patch plasty (TAPP): Incidence, risk factors, and
Seroma happens to be the frequent complexity of TAPP and TEP preventive measures. Surg Endosc 2018;32:2222–2231. DOI: 10.1007/
6
and can easily orchestrate a dreaded mesh infection. Mesh infection s00464-017-5912-3.
World Journal of Laparoscopic Surgery, Volume 16 Issue 1 (January–April 2023) 55