
Page 22 - World Journal of Laparoscopic Surgery
P. 22
Transillumination in Laparoscopic Hernia Repair
surgeon’s confusion between the desire to insert it as lateral as The surgeon and the assistant are positioned on the left side,
possible, and the fear from injuring the colon or other adherent the assistant may change his position to the right or to the left
tissues. This can be achieved by extracorporeal transillumination of side of the surgeon according to the stage. The laparoscopy tower
the anterior abdominal wall before insertion of the primary trocar, is positioned on the right side of the patient. Pneumoperitoneum is
thus exploring and delineating whether the abdominal wall harbors induced with a Veress needle 3 cm under the left costal margin on
any underlying tissues, and accordingly trying to visualize what is the mid-clavicular line, initial pressure for insufflation is 15 mm Hg,
being performed rather than doing it blindly. We recommend the after the insertion of the first trocar it will be reduced to 12 mm Hg,
implementation of extracorporeal abdominal transillumination The first trocar (the visual trocar) is 10 mm in diameter, it is
before insertion of the primary trocar as a protective step aiming to introduced at the defect level in the anterior axillary line in group II,
eliminate the incidence of gastrointestinal or other tissue injuries. and it is positioned according to the impression obtained from the
transillumination in group I. The 5-mm working instrument trocar is
MAterIAls And Methods introduced under vision below the left costal margin as laterally as
This is a single-center, blinded outcome assessment, two-group possible. The peritoneal cavity is explored. The hernia sac content
parallel-design study conducted at the department of surgery, is then reduced, and the peritoneum around the hernia defect
Al Jedaani hospital (private hospital in Jeddah, Saudi Arabia). The is cleared circumferentially for a distance of 5 cm to allow direct
research and ethics review committee at the hospital gave approval contact of the mesh to the parietal peritoneum.
to this study. Patients’ enrollment was carried out between March We used Symbotex™ composite mesh, it is designed extracor-
2018 and June 2019. Patients’ ages ranged from 20 to 65 years, poreally to cover the defect with a circumferential 5-cm overlay
undergoing elective laparoscopic midline ventral hernia repair with margin. The parietal surface of the mesh is stitched with 4 corners
a defect of 2–7 cm in diameter, were eligible for inclusion. Midline absorbable sutures with long threads. The mesh is placed on the
ventral hernia was defined as an abdominal wall hernia located skin, centered and marked over the defect, next to each knot a
between the xiphoid process and the symphysis pubis. Exclusion mini-incision of 2 mm is done on the skin, where the transfascial
criteria were: complicated hernias for emergency surgery, severe closure needle is passed to pull out the sutures. The mesh is damped
comorbidities, pregnancy, and body mass index (BMI) exceeding in saline solution, the mesh is rolled with the polyester outer side
2
35 kg/m . Informed consent was obtained from all patients. the mesh is held with the atraumatic instrument, and it is introduced
The patients were randomized into two arms as follows: into the abdominal cavity through the 10-mm port, unfolded, and
Laparoscopic repair using transillumination step before inserting applied to the defect with the bioabsorbable collagen film to the
the primary trocar (group I) and laparoscopic repair only visceral side, the transfascial closure needle is passed in the four
(group II). Randomization for eligible patients was done by using skin incisions to pull out the threads with a distance of approxi-
computerized simple sequence randomization. Blocking was not mately 5 mm between the 2 threads at each corner, the abdomen
done in this study. Random allocation was hidden by using sealed is deflated to 8 mm Hg pressure. Threads are tied and buried in
envelopes with sequential numbers. Each envelope was opened the subcutaneous plane. Helical absorbable fasteners are used
later on sequentially just before the operation. by the tacker fixation device to attach the whole area of the mesh
to the abdominal wall, and a compression bandage is applied to
Operative Technique the defect. The patients were discharged 24–48 hours. Compres-
The procedure is performed under general anesthesia, a sion bandage could be changed but maintained for 7–10 days to
prophylactic dose of antibiotic is administered upon induction. The prevent parietal seroma.
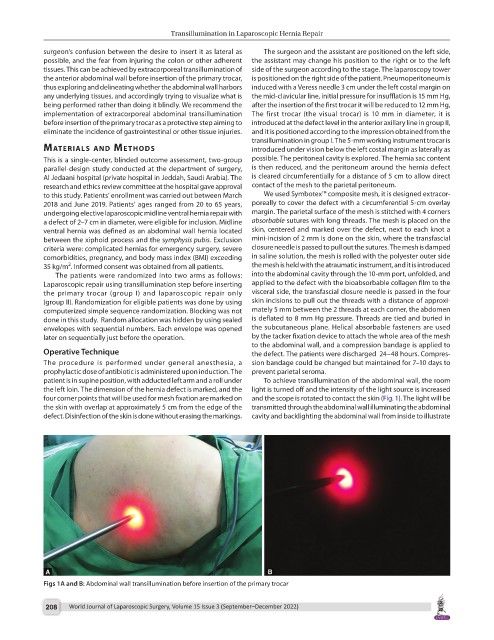
patient is in supine position, with adducted left arm and a roll under To achieve transillumination of the abdominal wall, the room
the left loin. The dimension of the hernia defect is marked, and the light is turned off and the intensity of the light source is increased
four corner points that will be used for mesh fixation are marked on and the scope is rotated to contact the skin (Fig. 1). The light will be
the skin with overlap at approximately 5 cm from the edge of the transmitted through the abdominal wall illuminating the abdominal
defect. Disinfection of the skin is done without erasing the markings. cavity and backlighting the abdominal wall from inside to illustrate
Figs 1A and B: Abdominal wall transillumination before insertion of the primary trocar
208 World Journal of Laparoscopic Surgery, Volume 15 Issue 3 (September–December 2022)