
Page 41 - World Journal of Laparoscopic Surgery
P. 41
Preoperative Scoring System to Predict Difficult LC
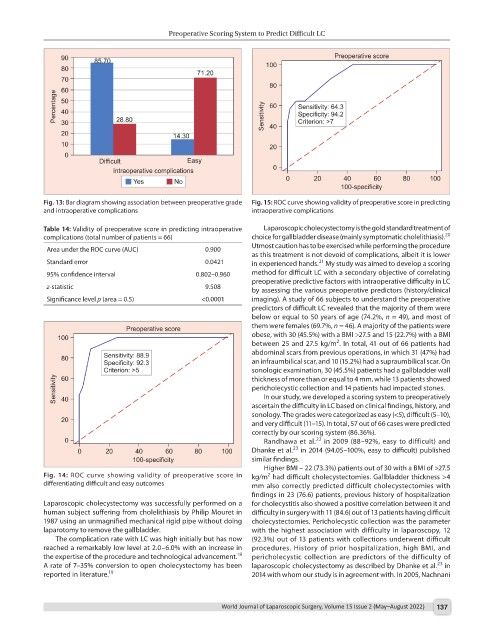
Fig. 13: Bar diagram showing association between preoperative grade Fig. 15: ROC curve showing validity of preoperative score in predicting
and intraoperative complications intraoperative complications
Table 14: Validity of preoperative score in predicting intraoperative Laparoscopic cholecystectomy is the gold standard treatment of
20
complications (total number of patients = 66) choice for gallbladder disease (mainly symptomatic cholelithiasis).
Utmost caution has to be exercised while performing the procedure
Area under the ROC curve (AUC) 0.900
as this treatment is not devoid of complications, albeit it is lower
21
Standard error 0.0421 in experienced hands. My study was aimed to develop a scoring
95% confidence interval 0.802–0.960 method for difficult LC with a secondary objective of correlating
preoperative predictive factors with intraoperative difficulty in LC
z-statistic 9.508 by assessing the various preoperative predictors (history/clinical
Significance level p (area = 0.5) <0.0001 imaging). A study of 66 subjects to understand the preoperative
predictors of difficult LC revealed that the majority of them were
below or equal to 50 years of age (74.2%, n = 49), and most of
them were females (69.7%, n = 46). A majority of the patients were
obese, with 30 (45.5%) with a BMI >27.5 and 15 (22.7%) with a BMI
2
between 25 and 27.5 kg/m . In total, 41 out of 66 patients had
abdominal scars from previous operations, in which 31 (47%) had
an infraumbilical scar, and 10 (15.2%) had a supraumbilical scar. On
sonologic examination, 30 (45.5%) patients had a gallbladder wall
thickness of more than or equal to 4 mm, while 13 patients showed
pericholecystic collection and 14 patients had impacted stones.
In our study, we developed a scoring system to preoperatively
ascertain the difficulty in LC based on clinical findings, history, and
sonology. The grades were categorized as easy (<5), difficult (5–10),
and very difficult (11–15). In total, 57 out of 66 cases were predicted
correctly by our scoring system (86.36%).
22
Randhawa et al. in 2009 (88–92%, easy to difficult) and
23
Dhanke et al. in 2014 (94.05–100%, easy to difficult) published
similar findings.
Higher BMI – 22 (73.3%) patients out of 30 with a BMI of >27.5
Fig. 14: ROC curve showing validity of preoperative score in kg/m had difficult cholecystectomies. Gallbladder thickness >4
2
differentiating difficult and easy outcomes mm also correctly predicted difficult cholecystectomies with
findings in 23 (76.6) patients, previous history of hospitalization
Laparoscopic cholecystectomy was successfully performed on a for cholecystitis also showed a positive correlation between it and
human subject suffering from cholelithiasis by Philip Mouret in difficulty in surgery with 11 (84.6) out of 13 patients having difficult
1987 using an unmagnified mechanical rigid pipe without doing cholecystectomies. Pericholecystic collection was the parameter
laparotomy to remove the gallbladder. with the highest association with difficulty in laparoscopy, 12
The complication rate with LC was high initially but has now (92.3%) out of 13 patients with collections underwent difficult
reached a remarkably low level at 2.0–6.0% with an increase in procedures. History of prior hospitalization, high BMI, and
18
the expertise of the procedure and technological advancement. pericholecystic collection are predictors of the difficulty of
23
A rate of 7–35% conversion to open cholecystectomy has been laparoscopic cholecystectomy as described by Dhanke et al. in
reported in literature. 19 2014 with whom our study is in agreement with. In 2005, Nachnani
World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022) 137