
Page 36 - World Journal of Laparoscopic Surgery
P. 36
Preoperative Scoring System to Predict Difficult LC
Advancing age, ethnic background, family history, female
gender, and or genetics are some risk factors for cholelithiasis
which cannot be modified. The risks which can be modified for
gallstones are an idle lifestyle, sudden weight loss, and obesity. A
rise in gallstone frequency is expected with the rising epidemic
of obesity and its associated metabolic syndrome. Drugs such
as thiazide diuretics, ceftriaxone, octreotide, pregnancy, total
parenteral nutrition, and fasting are some of the risk factors
for biliary sludge. Chronic hemolysis, cirrhosis, and Crohn’s
disease are a few risk factors for the formation of black pigment
stones. 10
The first cholecystectomy was performed on a patient who
suffered from cholelithiasis by Carl Johann August Langenbuch, who
pioneered Cholecystectomy in 1882. It has since been considered
the surgery of choice for gallstone disease (cholelithiasis). The
gold standard for treatment of most of the gallbladder diseases
is considered to be LC. Shorter duration of hospital stay, less
postoperative pain, faster return of bowel function, better cosmesis,
and also quicker return to full activity are some of the advantages
of LC.
Although LC is the gold standard, there are instances of
LC, when the surgery becomes difficult. There are instances of
surgery taking a longer than expected duration with bile/stone
spillage, iatrogenic injury of common bile/hepatic duct, and
thickly adherent gallbladder, and occasionally some surgeries
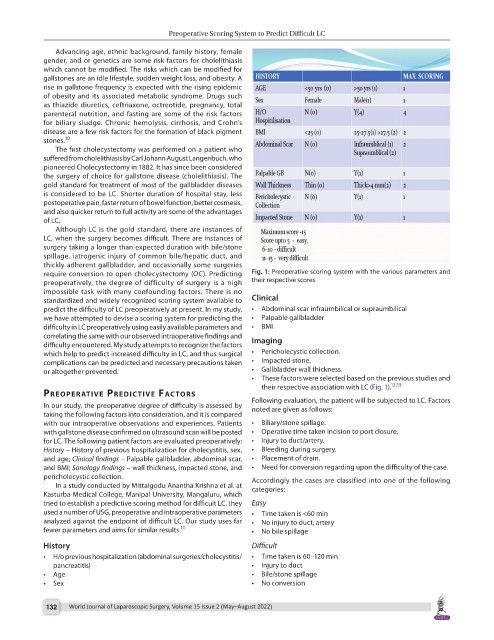
require conversion to open cholecystectomy (OC). Predicting Fig. 1: Preoperative scoring system with the various parameters and
preoperatively, the degree of difficulty of surgery is a nigh their respective scores
impossible task with many confounding factors. There is no
standardized and widely recognized scoring system available to Clinical
predict the difficulty of LC preoperatively at present. In my study, • Abdominal scar infraumbilical or supraumbilical
we have attempted to devise a scoring system for predicting the • Palpable gallbladder
difficulty in LC preoperatively using easily available parameters and • BMI
correlating the same with our observed intraoperative findings and
difficulty encountered. My study attempts to recognize the factors Imaging
which help to predict increased difficulty in LC, and thus surgical • Pericholecystic collection.
complications can be predicted and necessary precautions taken • Impacted stone.
or altogether prevented. • Gallbladder wall thickness.
• These factors were selected based on the previous studies and
their respective association with LC (Fig. 1). 12,13
PreoPerAtIve PredIctIve FActors
In our study, the preoperative degree of difficulty is assessed by Following evaluation, the patient will be subjected to LC. Factors
noted are given as follows:
taking the following factors into consideration, and it is compared
with our intraoperative observations and experiences. Patients • Biliary/stone spillage.
with gallstone disease confirmed on ultrasound scan will be posted • Operative time taken incision to port closure.
for LC. The following patient factors are evaluated preoperatively: • Injury to duct/artery.
History – History of previous hospitalization for cholecystitis, sex, • Bleeding during surgery.
and age; Clinical findings – Palpable gallbladder, abdominal scar, • Placement of drain.
and BMI; Sonology findings – wall thickness, impacted stone, and • Need for conversion regarding upon the difficulty of the case.
pericholecystic collection. Accordingly the cases are classified into one of the following
In a study conducted by Mittalgodu Anantha Krishna et al. at categories:
Kasturba Medical College, Manipal University, Mangaluru, which
tried to establish a predictive scoring method for difficult LC, they Easy
used a number of USG, preoperative and intraoperative parameters • Time taken is <60 min
analyzed against the endpoint of difficult LC. Our study uses far • No injury to duct, artery
fewer parameters and aims for similar results. 11 • No bile spillage
History Difficult
• H/o previous hospitalization (abdominal surgeries/cholecystitis/ • Time taken is 60–120 min
pancreatitis) • Injury to duct
• Age • Bile/stone spillage
• Sex • No conversion
132 World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022)