
Page 8 - World Journal of Laparoscopic Surgery
P. 8
Conversion of LC to Open Surgery
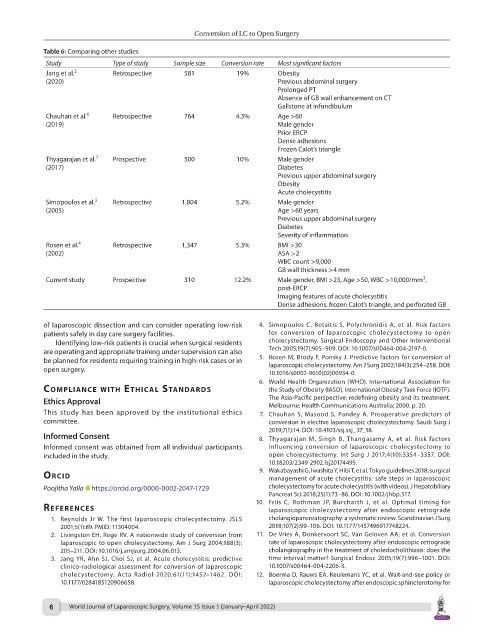
Table 6: Comparing other studies
Study Type of study Sample size Conversion rate Most significant factors
Jang et al. 2 Retrospective 581 19% Obesity
(2020) Previous abdominal surgery
Prolonged PT
Absence of GB wall enhancement on CT
Gallstone at infundibulum
Chauhan et al. 6 Retrospective 764 4.3% Age >60
(2019) Male gender
Prior ERCP
Dense adhesions
Frozen Calot’s triangle
Thyagarajan et al. 7 Prospective 500 10% Male gender
(2017) Diabetes
Previous upper abdominal surgery
Obesity
Acute cholecystitis
Simopoulos et al. 3 Retrospective 1,804 5.2% Male gender
(2005) Age >60 years
Previous upper abdominal surgery
Diabetes
Severity of inflammation
Rosen et al. 4 Retrospective 1,347 5.3% BMI >30
(2002) ASA >2
WBC count >9,000
GB wall thickness >4 mm
3
Current study Prospective 310 12.2% Male gender, BMI >23, Age >50, WBC >10,000/mm ,
post-ERCP
Imaging features of acute cholecystitis
Dense adhesions, frozen Calot’s triangle, and perforated GB
of laparoscopic dissection and can consider operating low-risk 4. Simopoulos C, Botaitis S, Polychronidis A, et al. Risk factors
patients safely in day care surgery facilities. for conversion of laparoscopic cholecystectomy to open
Identifying low-risk patients is crucial when surgical residents cholecystectomy. Surgical Endoscopy and Other Interventional
are operating and appropriate training under supervision can also Tech 2005;19(7):905–909. DOI: 10.1007/s00464-004-2197-0.
be planned for residents requiring training in high-risk cases or in 5. Rosen M, Brody F, Ponsky J. Predictive factors for conversion of
open surgery. laparoscopic cholecystectomy. Am J Surg 2002;184(3):254–258. DOI:
10.1016/s0002-9610(02)00934-0.
6. World Health Organization (WHO). International Association for
coMplIAnce wIth ethIcAl stAndArds the Study of Obesity (IASO), International Obesity Task Force (IOTF).
Ethics Approval The Asia-Pacific perspective: redefining obesity and its treatment.
Melbourne: Health Communications Australia; 2000. p. 20.
This study has been approved by the institutional ethics 7. Chauhan S, Masood S, Pandey A. Preoperative predictors of
committee. conversion in elective laparoscopic cholecystectomy. Saudi Surg J
2019;7(1):14. DOI: 10.4103/ssj.ssj_37_18.
Informed Consent 8. Thyagarajan M, Singh B, Thangasamy A, et al. Risk factors
Informed consent was obtained from all individual participants influencing conversion of laparoscopic cholecystectomy to
included in the study. open cholecystectomy. Int Surg J 2017;4(10):3354–3357. DOI:
10.18203/2349-2902.isj20174495.
9. Wakabayashi G, Iwashita Y, Hibi T, et al. Tokyo guidelines 2018: surgical
orcId management of acute cholecystitis: safe steps in laparoscopic
Poojitha Yalla https://orcid.org/0000-0002-2047-1729 cholecystectomy for acute cholecystitis (with videos). J Hepatobiliary
Pancreat Sci 2018;25(1):73–86. DOI: 10.1002/jhbp.517.
10. Friis C, Rothman JP, Burcharth J, et al. Optimal timing for
references laparoscopic cholecystectomy after endoscopic retrograde
1. Reynolds Jr W. The first laparoscopic cholecystectomy. JSLS cholangiopancreatography: a systematic review. Scandinavian J Surg
2001;5(1):89. PMID: 11304004. 2018;107(2):99–106. DOI: 10.1177/1457496917748224.
2. Livingston EH, Rege RV. A nationwide study of conversion from 11. De Vries A, Donkervoort SC, Van Geloven AA, et al. Conversion
laparoscopic to open cholecystectomy. Am J Surg 2004;188(3): rate of laparoscopic cholecystectomy after endoscopic retrograde
205–211. DOI: 10.1016/j.amjsurg.2004.06.013. cholangiography in the treatment of choledocholithiasis: does the
3. Jang YR, Ahn SJ, Choi SJ, et al. Acute cholecystitis: predictive time interval matter? Surgical Endosc 2005;19(7):996–1001. DOI:
clinico-radiological assessment for conversion of laparoscopic 10.1007/s00464-004-2206-3.
cholecystectomy. Acta Radiol 2020;61(11):1452–1462. DOI: 12. Boerma D, Rauws EA, Keulemans YC, et al. Wait-and-see policy or
10.1177/0284185120906658. laparoscopic cholecystectomy after endoscopic sphincterotomy for
6 World Journal of Laparoscopic Surgery, Volume 15 Issue 1 (January–April 2022)