
Page 48 - WJOLS
P. 48
World Journal of Laparoscopic Surgery, September-December 2008;1(3):46-48
Minaya Bravo et al
Two Rare Cases of Intrahepatic Subcapsular
Hematoma After Laparoscopic Cholecystectomy
Minaya Bravo, González AM, González E, Cardeñoso Payo P, Ortiz Aguilar M, Larrañaga E
La Princesa Hospital, Calle Diego de León, n 62. 28006, Madrid, Spain
Abstract On the fifth day after surgery, the patient had right upper
quadrant pain, nauseas and vomits. Blood test showed a light
The appearance of subcapsular hematoma liver after a laparoscopic
cholecystectomy is a complication few studied and few cases have decrease of hemoglobin: 9.6 g/L. An ultrasound was made and
been described in the literature. Some of them have been connected to no lesions were revealed.
administration of ketorolac during and after surgery, because of its After 24 hours, the patient showed hemodynamic instability,
anti-platelet activity. But other factors such as hemangioma or hypotension and tachycardia, and blood test: hemoglobin of
lacerations could play an important role as well. In addition, the 4.5g/L, and increase of liver enzymes: GOT 5782, GPT 367 and
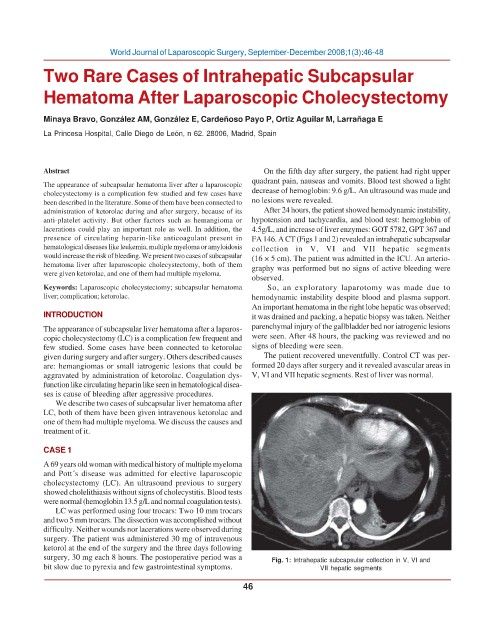
presence of circulating heparin-like anticoagulant present in FA 146. A CT (Figs 1 and 2) revealed an intrahepatic subcapsular
hematological diseases like leukemia, multiple myeloma or amyloidosis collection in V, VI and VII hepatic segments
would increase the risk of bleeding. We present two cases of subcapsular (16 × 5 cm). The patient was admitted in the ICU. An arterio-
hematoma liver after laparoscopic cholecystectomy, both of them graphy was performed but no signs of active bleeding were
were given ketorolac, and one of them had multiple myeloma.
observed.
Keywords: Laparoscopic cholecystectomy; subcapsular hematoma So, an exploratory laparotomy was made due to
liver; complication; ketorolac. hemodynamic instability despite blood and plasma support.
An important hematoma in the right lobe hepatic was observed;
INTRODUCTION it was drained and packing, a hepatic biopsy was taken. Neither
The appearance of subcapsular liver hematoma after a laparos- parenchymal injury of the gallbladder bed nor iatrogenic lesions
copic cholecystectomy (LC) is a complication few frequent and were seen. After 48 hours, the packing was reviewed and no
few studied. Some cases have been connected to ketorolac signs of bleeding were seen.
given during surgery and after surgery. Others described causes The patient recovered uneventfully. Control CT was per-
are: hemangiomas or small iatrogenic lesions that could be formed 20 days after surgery and it revealed avascular areas in
aggravated by administration of ketorolac. Coagulation dys- V, VI and VII hepatic segments. Rest of liver was normal.
function like circulating heparin like seen in hematological disea-
ses is cause of bleeding after aggressive procedures.
We describe two cases of subcapsular liver hematoma after
LC, both of them have been given intravenous ketorolac and
one of them had multiple myeloma. We discuss the causes and
treatment of it.
CASE 1
A 69 years old woman with medical history of multiple myeloma
and Pott´s disease was admitted for elective laparoscopic
cholecystectomy (LC). An ultrasound previous to surgery
showed cholelithiasis without signs of cholecystitis. Blood tests
were normal (hemoglobin 13.5 g/L and normal coagulation tests).
LC was performed using four trocars: Two 10 mm trocars
and two 5 mm trocars. The dissection was accomplished without
difficulty. Neither wounds nor lacerations were observed during
surgery. The patient was administered 30 mg of intravenous
ketorol at the end of the surgery and the three days following
surgery, 30 mg each 8 hours. The postoperative period was a Fig. 1: Intrahepatic subcapsular collection in V, VI and
bit slow due to pyrexia and few gastrointestinal symptoms. VII hepatic segments
46