
Page 29 - World Journal of Laparoscopic Surgery
P. 29
Cromwell HM Mwakirungu
Myomectomy can be performed either through an abdominal MATERIAL AND METHODS
incision (laparotomy) or through small holes made using canulas A literature search was performed using Medline, Highwire
and trocars and using a special telescope to perform the surgery press, Springerlink and the Google search engine. The following
(laparoscopic). After laparoscopic myomectomy, the myomas search terms were used: myoma, myomectomy, laparoscopy,
are removed from inside the abdomen by either an instrument laparotomy. GnRH analogues and hysteroscopy. 1400 citations
called a morcillator, or through an incision through the posterior were found in all. Selected papers were screened for further
cul de sac of Douglas and through the vagina. references. Criteria for selection of literature were the number of
Hysteroscopic myomectomy can also be done for
endometrial or submucous myomas. cases (excluded if less than 20), methods of analysis (statistical
or nonstatistical), operative procedure (only universally
accepted procedures were selected) and the institution where
AIMS AND OBJECTIVES
the study was done (specialized institutions for laparoscopic
The aim of the study was to compare whether there are any surgery.
advantages by doing laparoscopic myomectomy over the
conventional ‘open’ myomectomy. The following parameters
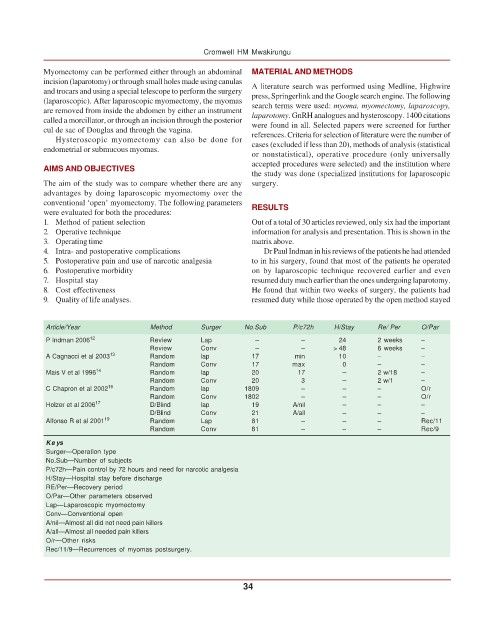
were evaluated for both the procedures: RESULTS
1. Method of patient selection Out of a total of 30 articles reviewed, only six had the important
2. Operative technique information for analysis and presentation. This is shown in the
3. Operating time matrix above.
4. Intra- and postoperative complications Dr Paul Indman in his reviews of the patients he had attended
5. Postoperative pain and use of narcotic analgesia to in his surgery, found that most of the patients he operated
6. Postoperative morbidity on by laparoscopic technique recovered earlier and even
7. Hospital stay resumed duty much earlier than the ones undergoing laparotomy.
8. Cost effectiveness He found that within two weeks of surgery, the patients had
9. Quality of life analyses. resumed duty while those operated by the open method stayed
Article/Year Method Surger No.Sub P/c72h H/Stay Re/ Per O/Par
P Indman 2006 12 Review Lap – – 24 2 weeks –
Review Conv – – > 48 6 weeks –
A Cagnacci et al 2003 13 Random lap 17 min 10 – –
Random Conv 17 max 0 – –
Mais V et al 1996 14 Random lap 20 17 – 2 w/18 –
Random Conv 20 3 – 2 w/1 –
C Chapron et al 2002 16 Random lap 1809 – – – O/r
Random Conv 1802 – – – O/r
Holzer et al 2006 17 D/Blind lap 19 A/nil – – –
D/Blind Conv 21 A/all – – –
Alfonso R et al 2001 19 Random Lap 81 – – – Rec/11
Random Conv 81 – – – Rec/9
Ke ys
Surger—Operation type
No.Sub—Number of subjects
P/c72h—Pain control by 72 hours and need for narcotic analgesia
H/Stay—Hospital stay before discharge
RE/Per—Recovery period
O/Par—Other parameters observed
Lap—Laparoscopic myomectomy
Conv—Conventional open
A/nil—Almost all did not need pain killers
A/all—Almost all needed pain killers
O/r—Other risks
Rec/11/9—Recurrences of myomas postsurgery.
34