
Page 38 - World Journal of Laparoscopic Surgery
P. 38
Different Port Closure Techniques in Laparoscopy Surgery
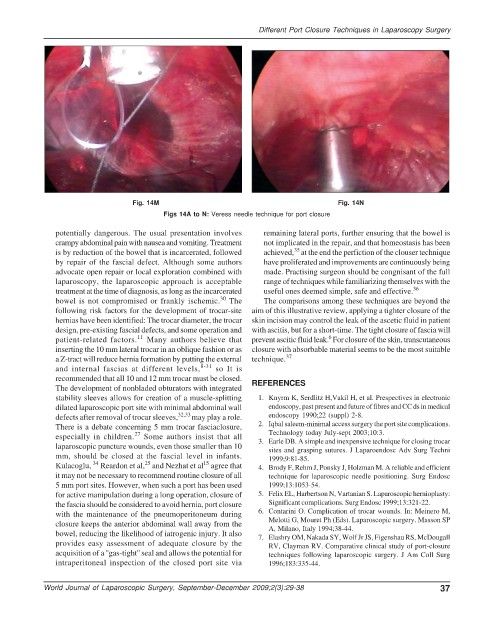
Fig. 14M Fig. 14N
Figs 14A to N: Veress needle technique for port closure
potentially dangerous. The usual presentation involves remaining lateral ports, further ensuring that the bowel is
crampy abdominal pain with nausea and vomiting. Treatment not implicated in the repair, and that homeostasis has been
35
is by reduction of the bowel that is incarcerated, followed achieved, at the end the perfiction of the clouser technique
by repair of the fascial defect. Although some authors have proliferated and improvements are continuously being
advocate open repair or local exploration combined with made. Practising surgeon should be congnisant of the full
laparoscopy, the laparoscopic approach is acceptable range of techniques while familiarizing themselves with the
treatment at the time of diagnosis, as long as the incarcerated useful ones deemed simple, safe and effective. 36
30
bowel is not compromised or frankly ischemic. The The comparisons among these techniques are beyond the
following risk factors for the development of trocar-site aim of this illustrative review, applying a tighter closure of the
hernias have been identified: The trocar diameter, the trocar skin incision may control the leak of the ascetic fluid in patient
design, pre-existing fascial defects, and some operation and with ascitis, but for a short-time. The tight closure of fascia will
11
6
patient-related factors. Many authors believe that prevent ascitic fluid leak. For closure of the skin, transcutaneous
inserting the 10 mm lateral trocar in an oblique fashion or as closure with absorbable material seems to be the most suitable
a Z-tract will reduce hernia formation by putting the external technique. 37
and internal fascias at different levels, 8-31 so It is
recommended that all 10 and 12 mm trocar must be closed. REFERENCES
The development of nonbladed obturators with integrated
stability sleeves allows for creation of a muscle-splitting 1. Knyrm K, Serdlitz H,Vakil H, et al. Prespectives in electronic
dilated laparoscopic port site with minimal abdominal wall endoscopy, past present and future of fibres and CC ds in medical
defects after removal of trocar sleeves, 32,33 may play a role. endoscopy 1990;22 (suppl) 2-8.
There is a debate concerning 5 mm trocar fasciaclosure, 2. Iqbal saleem-minimal access surgery the port site complications.
Technology today July-sept 2003;10:3.
27
especially in children. Some authors insist that all 3. Earle DB. A simple and inexpensive technique for closing trocar
laparoscopic puncture wounds, even those smaller than 10 sites and grasping sutures. J Laparoendosc Adv Surg Techni
mm, should be closed at the fascial level in infants. 1999;9:81-85.
34
25
15
Kulacoglu, Reardon et al, and Nezhat et al agree that 4. Brody F, Rehm J, Ponsky J, Holzman M. A reliable and efficient
it may not be necessary to recommend routine closure of all technique for laparoscopic needle positioning. Surg Endosc
5 mm port sites. However, when such a port has been used 1999;13:1053-54.
for active manipulation during a long operation, closure of 5. Felix EL, Harbertson N, Vartanian S. Laparoscopic hernioplasty:
the fascia should be considered to avoid hernia, port closure Significant complications. Surg Endosc 1999;13:321-22.
with the maintenance of the pneumoperitoneum during 6. Contarini O. Complication of trocar wounds. In: Meinero M,
closure keeps the anterior abdominal wall away from the Melotti G, Mouret Ph (Eds). Laparoscopic surgery. Masson SP
A, Milano, Italy 1994;38-44.
bowel, reducing the likelihood of iatrogenic injury. It also 7. Elashry OM, Nakada SY, Wolf Jr JS, Figenshau RS, McDougall
provides easy assessment of adequate closure by the RV, Clayman RV. Comparative clinical study of port-closure
acquisition of a ''gas-tight'' seal and allows the potential for techniques following laparoscopic surgery. J Am Coll Surg
intraperitoneal inspection of the closed port site via 1996;183:335-44.
World Journal of Laparoscopic Surgery, September-December 2009;2(3):29-38 37