
Page 33 - World Journal of Laparoscopic Surgery
P. 33
Majid A Hamood
passed into the abdomen until the olive is visible below the
peritoneum. The instrument is then positioned in a plane
perpendicular to the trocar incision to expose the needle and
pass it through the peritoneum and fascia until it exits the skin
incision.The end of the suture is grasped and tagged with
ahemostat. The needle is dropped back into the olive, and the
instrument is rotated 180°. The olive is again dropped to expose
the needle, which is again passed through the peritoneum and
fascia. After removal of the Endo-Judge, the suture is tied,
creating a secure, airtight fascial and peritoneal closure.
24
The 2 mm trocar technique. Reardon et al. A 2 mm trocar
and sleeve are introduced adjacent to the port whose entry site
will be closed. A monofilamentheavy-gauge suture with the
needle removed is passed through the lumen of the 2 mm sleeve.
The 2 mm sleeve is then removed over the suture, after which
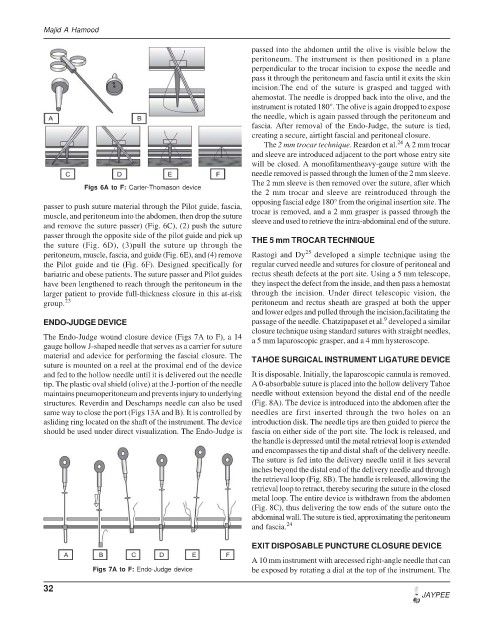
Figs 6A to F: Carter-Thomason device
the 2 mm trocar and sleeve are reintroduced through the
opposing fascial edge 180° from the original insertion site. The
passer to push suture material through the Pilot guide, fascia, trocar is removed, and a 2 mm grasper is passed through the
muscle, and peritoneum into the abdomen, then drop the suture sleeve and used to retrieve the intra-abdominal end of the suture.
and remove the suture passer) (Fig. 6C), (2) push the suture
passer through the opposite side of the pilot guide and pick up THE 5 mm TROCAR TECHNIQUE
the suture (Fig. 6D), (3)pull the suture up through the
25
peritoneum, muscle, fascia, and guide (Fig. 6E), and (4) remove Rastogi and Dy developed a simple technique using the
the Pilot guide and tie (Fig. 6F). Designed specifically for regular curved needle and sutures for closure of peritoneal and
bariatric and obese patients. The suture passer and Pilot guides rectus sheath defects at the port site. Using a 5 mm telescope,
have been lengthened to reach through the peritoneum in the they inspect the defect from the inside, and then pass a hemostat
larger patient to provide full-thickness closure in this at-risk through the incision. Under direct telescopic vision, the
group. 23 peritoneum and rectus sheath are grasped at both the upper
and lower edges and pulled through the incision,facilitating the
9
ENDO-JUDGE DEVICE passage of the needle. Chatzipapaset et al. developed a similar
closure technique using standard sutures with straight needles,
The Endo-Judge wound closure device (Figs 7A to F), a 14 a 5 mm laparoscopic grasper, and a 4 mm hysteroscope.
gauge hollow J-shaped needle that serves as a carrier for suture
material and adevice for performing the fascial closure. The TAHOE SURGICAL INSTRUMENT LIGATURE DEVICE
suture is mounted on a reel at the proximal end of the device
and fed to the hollow needle until it is delivered out the needle It is disposable. Initially, the laparoscopic cannula is removed.
tip. The plastic oval shield (olive) at the J-portion of the needle A 0-absorbable suture is placed into the hollow delivery Tahoe
maintains pneumoperitoneum and prevents injury to underlying needle without extension beyond the distal end of the needle
structures. Reverdin and Deschamps needle can also be used (Fig. 8A). The device is introduced into the abdomen after the
same way to close the port (Figs 13A and B). It is controlled by needles are first inserted through the two holes on an
asliding ring located on the shaft of the instrument. The device introduction disk. The needle tips are then guided to pierce the
should be used under direct visualization. The Endo-Judge is fascia on either side of the port site. The lock is released, and
the handle is depressed until the metal retrieval loop is extended
and encompasses the tip and distal shaft of the delivery needle.
The suture is fed into the delivery needle until it lies several
inches beyond the distal end of the delivery needle and through
the retrieval loop (Fig. 8B). The handle is released, allowing the
retrieval loop to retract, thereby securing the suture in the closed
metal loop. The entire device is withdrawn from the abdomen
(Fig. 8C), thus delivering the tow ends of the suture onto the
abdominal wall. The suture is tied, approximating the peritoneum
and fascia. 24
EXIT DISPOSABLE PUNCTURE CLOSURE DEVICE
A 10 mm instrument with arecessed right-angle needle that can
Figs 7A to F: Endo-Judge device be exposed by rotating a dial at the top of the instrument. The
32
JAYPEE