
Page 32 - World Journal of Laparoscopic Surgery
P. 32
Different Port Closure Techniques in Laparoscopy Surgery
holding the suture, is reinserted at the next point and, with the
use of the forceps, the free intra-abdominal edge of the suture
is locked through the loop that has been created. This maneuver
is repeated another three times until the purse string is fashioned.
In the final step, the suture edge, which is pulled by the last
loop, and the needle are withdrawn outside the abdomen near
the site of first needle insertion, and both edges of the suture
are tied up onto the fascia, angiocath needle to perform the
same closure technique (Fig. 3C). The large 10 mm trocar is
removed, and the pneumoperitoneum is maintained in all
abdominal trocar wounds 10 mm or larger simply by placement
of a gloved finger over the top of the wound. A 14 gauge
angiocath needle with the sheath removed is preloaded with a
50 cm length of 0- braided polyglactin suture. The angiocath
and suture are inserted through all fascia layers on one side of
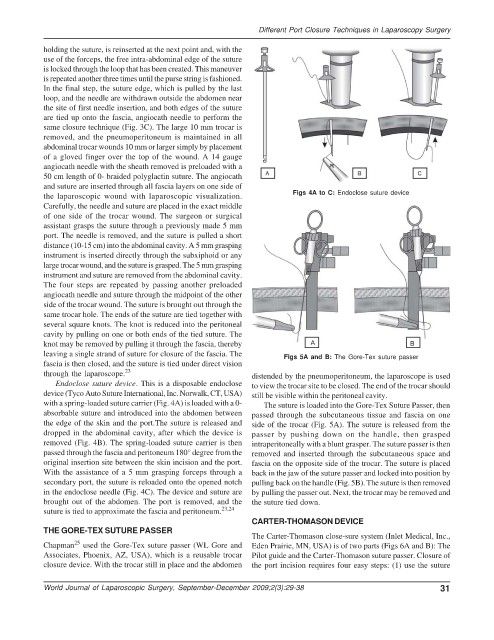
the laparoscopic wound with laparoscopic visualization. Figs 4A to C: Endoclose suture device
Carefully, the needle and suture are placed in the exact middle
of one side of the trocar wound. The surgeon or surgical
assistant grasps the suture through a previously made 5 mm
port. The needle is removed, and the suture is pulled a short
distance (10-15 cm) into the abdominal cavity. A 5 mm grasping
instrument is inserted directly through the subxiphoid or any
large trocar wound, and the suture is grasped. The 5 mm grasping
instrument and suture are removed from the abdominal cavity.
The four steps are repeated by passing another preloaded
angiocath needle and suture through the midpoint of the other
side of the trocar wound. The suture is brought out through the
same trocar hole. The ends of the suture are tied together with
several square knots. The knot is reduced into the peritoneal
cavity by pulling on one or both ends of the tied suture. The
knot may be removed by pulling it through the fascia, thereby
leaving a single strand of suture for closure of the fascia. The Figs 5A and B: The Gore-Tex suture passer
fascia is then closed, and the suture is tied under direct vision
through the laparoscope. 23 distended by the pneumoperitoneum, the laparoscope is used
Endoclose suture device. This is a disposable endoclose to view the trocar site to be closed. The end of the trocar should
device (Tyco Auto Suture International, Inc. Norwalk, CT, USA) still be visible within the peritoneal cavity.
with a spring-loaded suture carrier (Fig. 4A) is loaded with a 0- The suture is loaded into the Gore-Tex Suture Passer, then
absorbable suture and introduced into the abdomen between passed through the subcutaneous tissue and fascia on one
the edge of the skin and the port.The suture is released and side of the trocar (Fig. 5A). The suture is released from the
dropped in the abdominal cavity, after which the device is passer by pushing down on the handle, then grasped
removed (Fig. 4B). The spring-loaded suture carrier is then intraperitoneally with a blunt grasper. The suture passer is then
passed through the fascia and peritoneum 180° degree from the removed and inserted through the subcutaneous space and
original insertion site between the skin incision and the port. fascia on the opposite side of the trocar. The suture is placed
With the assistance of a 5 mm grasping forceps through a back in the jaw of the suture passer and locked into position by
secondary port, the suture is reloaded onto the opened notch pulling back on the handle (Fig. 5B). The suture is then removed
in the endoclose needle (Fig. 4C). The device and suture are by pulling the passer out. Next, the trocar may be removed and
brought out of the abdomen. The port is removed, and the the suture tied down.
suture is tied to approximate the fascia and peritoneum. 23,24
CARTER-THOMASON DEVICE
THE GORE-TEX SUTURE PASSER
The Carter-Thomason close-sure system (Inlet Medical, Inc.,
25
Chapman used the Gore-Tex suture passer (WL Gore and Eden Prairie, MN, USA) is of two parts (Figs 6A and B): The
Associates, Phoenix, AZ, USA), which is a reusable trocar Pilot guide and the Carter-Thomason suture passer. Closure of
closure device. With the trocar still in place and the abdomen the port incision requires four easy steps: (1) use the suture
World Journal of Laparoscopic Surgery, September-December 2009;2(3):29-38 31