
Page 7 - World's Most Popular Laparoscopic Journal
P. 7
Nina Irawati
follicular carcinoma. Futher treatment was needed, and she to 11 mm Hg. A 10 mm, 0 degree endoscope was inserted
is now prepared for the completion of thyroidectomy endos- under its guidance. We inserted other 5 mm trocar
copically. respectively. The subcutaneous tunnel was further enlarged
with bipolar and hook equipment. The lateral border of
CASE ILLUSTRATION II
sternocleidomastoideus was dissected and omohyoid was
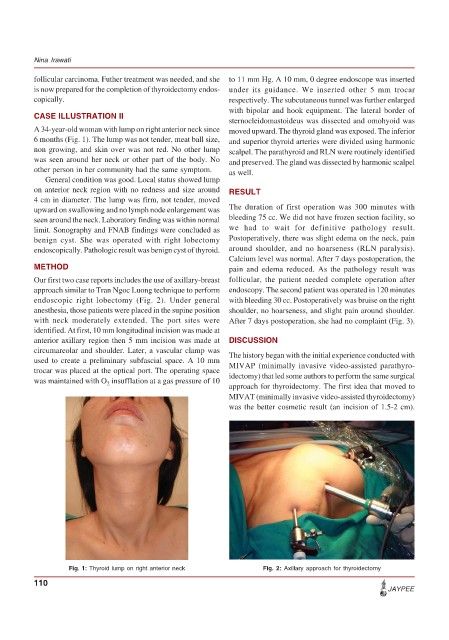
A 34-year-old woman with lump on right anterior neck since moved upward. The thyroid gland was exposed. The inferior
6 months (Fig. 1). The lump was not tender, meat ball size, and superior thyroid arteries were divided using harmonic
non growing, and skin over was not red. No other lump scalpel. The parathyroid and RLN were routinely identified
was seen around her neck or other part of the body. No and preserved. The gland was dissected by harmonic scalpel
other person in her community had the same symptom. as well.
General condition was good. Local status showed lump
on anterior neck region with no redness and size around RESULT
4 cm in diameter. The lump was firm, not tender, moved
upward on swallowing and no lymph node enlargement was The duration of first operation was 300 minutes with
seen around the neck. Laboratory finding was within normal bleeding 75 cc. We did not have frozen section facility, so
limit. Sonography and FNAB findings were concluded as we had to wait for definitive pathology result.
benign cyst. She was operated with right lobectomy Postoperatively, there was slight edema on the neck, pain
endoscopically. Pathologic result was benign cyst of thyroid. around shoulder, and no hoarseness (RLN paralysis).
Calcium level was normal. After 7 days postoperation, the
METHOD pain and edema reduced. As the pathology result was
Our first two case reports includes the use of axillary-breast follicular, the patient needed complete operation after
approach similar to Tran Ngoc Luong technique to perform endoscopy. The second patient was operated in 120 minutes
endoscopic right lobectomy (Fig. 2). Under general with bleeding 30 cc. Postoperatively was bruise on the right
anesthesia, those patients were placed in the supine position shoulder, no hoarseness, and slight pain around shoulder.
with neck moderately extended. The port sites were After 7 days postoperation, she had no complaint (Fig. 3).
identified. At first, 10 mm longitudinal incision was made at
anterior axillary region then 5 mm incision was made at DISCUSSION
circumareolar and shoulder. Later, a vascular clamp was The history began with the initial experience conducted with
used to create a preliminary subfascial space. A 10 mm
trocar was placed at the optical port. The operating space MIVAP (minimally invasive video-assisted parathyro-
idectomy) that led some authors to perform the same surgical
was maintained with O insufflation at a gas pressure of 10
2
approach for thyroidectomy. The first idea that moved to
MIVAT (minimally invasive video-assisted thyroidectomy)
was the better cosmetic result (an incision of 1.5-2 cm).
Fig. 1: Thyroid lump on right anterior neck Fig. 2: Axillary approach for thyroidectomy
110
JAYPEE