
Page 3 - World's Most Popular Laparoscopic Journal
P. 3
10.5005/jp-journals-10007-1094 WJOLS
ORIGINAL ARTICLE Laparoscopic Management of Billiary Ascariasis: A Case Report and Review of Literature
Laparoscopic Management of Biliary Ascariasis:
A Case Report and Review of Literature
2
1
1 Khairi Hajaji, Hisham Aljohary, Hassan Althani
1 Specialist, Department of General Surgery, Hamad General Hospital, Doha, Qatar
2 Consultant, Department of General and Vascular Surgery, Hamad General Hospital, Doha, Qatar
Abstract
Acute pancreatitis due to Ascaris lumbricoides is a known etiology but very rare in Qatar. The diagnosis can be difficult because of the
low index of suspicion. We report a case of 25-year-old Philippine patient living in Qatar who developed an acute pancreatitis due to
Ascaris lumbricoides and was diagnosed initially as biliary pancreatitis. We proceeded with laparoscopic cholecystectomy and intra-
operative cholangiogram which revealed Ascaris in the common bile duct. Transcystic extraction of a living worm from the common bile
duct was done. This is the first case report of acute pancreatitis due to Ascaris lumbricoides which had laparoscopic transcystic
extraction of a living worm from the common bile duct.
Background: Ascaris lumbricoides as etiology to acute pancreatitis has never been described in Qatar whereas in developing tropical
1
and subtropical areas, Ascaris lumbricoides is found in human gastrointestinal tract with greater prevalence. Although the infection can
be asymptomatic, in some cases the adult parasite can invade the biliary or pancreatic ducts and cause obstruction with development
2
of cholecystitis, cholangitis, and pancreatitis and hepatic abscesses. We report a case of a patient with biliary ascariasis induced acute
pancreatitis.
Conclusion: We recommend the use of this laparoscopic approach for treatment of such uncommon pathology, if surgical intervention
is needed. The differential diagnosis of pancreatitis should be expanded to include ascariasis in patients who come from population at
risk. Knowledge of clinical symptoms, complications, and diagnostic and therapeutic options are of paramount importance for all health
professionals.
Keywords: Biliary ascariasis, Laparoscopy in ascariasis, Management of ascariasis.
CLINICAL CASE was extracted carefully, placed in a plastic bag and removed
from the body (Fig. 2). A biliary drainage tube was not
A 25-year-old Philippine lady was admitted with right upper
quadrant pain of 2 days duration. Pain was accompanied used and the cystic duct incision was sutured and
by nausea, vomiting and radiation to the back. Laboratory cholecystectomy was finished laparoscopically. The
examinations demonstrated elevation of pancreatic amylase
(2980 IU/L), lipase (around 7000 IU/L); liver enzymes
were mildly elevated, with no jaundice. Ultrasonography
revealed thick-walled gallbladder filled with sludge and
stone; common bile duct (CBD) was mildly dilated.
Therefore, she was diagnosed as a case of biliary
pancreatitis. Medical treatment was started and on the
second day, the patient showed clinical and biochemistry
improvement, and the plan was to post her for laparoscopic
cholecystectomy and intraoperative cholangiogram in our
first elective operation list.
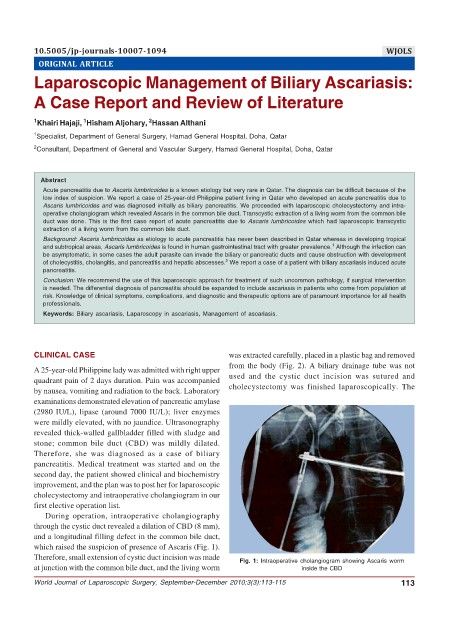
During operation, intraoperative cholangiography
through the cystic duct revealed a dilation of CBD (8 mm),
and a longitudinal filling defect in the common bile duct,
which raised the suspicion of presence of Ascaris (Fig. 1).
Therefore, small extension of cystic duct incision was made Fig. 1: Intraoperative cholangiogram showing Ascaris worm
at junction with the common bile duct, and the living worm inside the CBD
World Journal of Laparoscopic Surgery, September-December 2010;3(3):113-115 113